Sickle-cell disease is caused by a genetic mutation that leads to the production of Sickle hemoglobin, which affects the function of the red blood cells (RBCs) in the body. This mutation is inherited from the parents of an individual in an autosomal recessive pattern.
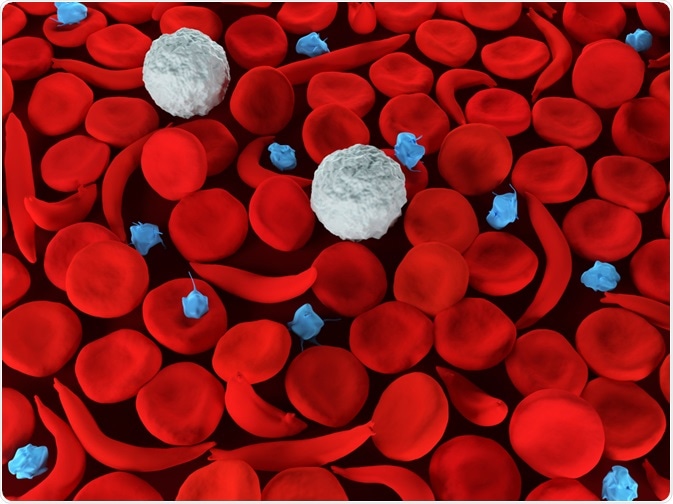
Image Credit: Meletios Verras / Shutterstock.com
Autosomal recessive inheritance
The hemoglobin S gene, which is responsible for altered hemoglobin and RBCs, is passed on when both parents must carry the gene mutation through a process known as an autosomal recessive pattern of inheritance.
Autosomal means that the mutation is not unique to the X or Y chromosome and can, therefore, affect males and females equally. Recessive means that the mutation must be present in both the father and the mother in order for the child to have sickle cell disease. When both parents are usually asymptomatic, they may not realize that they are carriers of the mutation.
When both parents are asymptomatic genetic carriers of the disease, each child has a chance of:
- 25% to acquire two defective genes and suffer from sickle cell disease.
- 50% to acquire one defected gene and develop a sickle cell disease trait, asymptomatic but a genetic carrier of the disease.
- 25% to inherit two normal genes and be unaffected by the genetic mutation and disease.
For each child that a couple has, the chance that the child will inherit the gene mutation remains the same, regardless of whether the previous children have been affected.
If only one parent is affected, the child may have a sickle cell trait. Children with a single gene mutation are usually healthy and do not typically experience significant side effects. However, they are a carrier of the condition and may pass the full disease on to any children if partnered with another person with sickle cell trait.
Sickle cell anaemia | Genetics | Biology | FuseSchool
Other genetic hemoglobin diseases
The genetic mutations involved in the pathophysiology of sickle cell disease are also related to the gene mutations of other conditions involving abnormal hemoglobin, such as thalassemia, hemoglobin C, hemoglobin D, and hemoglobin E.
For this reason, if one parent carries the Sickle hemoglobin gene mutation and the other carries another mutation related to hemoglobin, the risk of the child inheriting two gene mutations and suffering from the disease increases.
Genetic testing
It is possible for an individual to determine if they are affected by sickle cell disease and enable earlier interventions with the help of a blood test. This test screens for the presence of defective hemoglobin that is characteristic of the disease.
If there is a high level of defected hemoglobin, it is likely that the individual is affected and further investigations should be made. If there are some defective cells but are not widely spread, the individual is likely to have a sickle cell trait and be less likely to experience symptoms.
The majority of newborn babies are currently screened for sickle cell disease when they have the newborn blood spot test, also known as the heel prick test. This is particularly important for high-risk populations, such as those with family origins for regions where sickle cell disease is more common.
Pregnant women are also usually offered screening for the condition, particularly in areas where it is widespread. Alternatively, pregnant women may be asked to complete a questionnaire about the family origins to determine the risk of the parents carrying sickle hemoglobin mutation.
References
Further Reading
Last Updated: Apr 7, 2021
 Medicaid tries new approach with sickle cell: Companies get paid only if costly gene therapies work
Medicaid tries new approach with sickle cell: Companies get paid only if costly gene therapies work