This article is based on a poster originally authored by Bieke Soen, Leen Catrysse, Eva Van Lombergen, Manpreet Singh and Nithianandan Selliah.
CAR-T cell therapy has significantly advanced the treatment of blood cancers and shows promise for solid tumors. This immunotherapy employs genetically modified T-cells engineered to express a receptor that targets specific tumor antigens, thereby augmenting immune-driven tumor destruction.
Initially, treatments depended on autologous CAR T cells sourced from the patient. However, allogeneic CAR T cells, derived from healthy donors, are now progressing through clinical trials. Allogeneic CAR T cells offer an "off-the-shelf" alternative, providing quicker availability and greater scalability in production compared to autologous CAR T therapy. Nevertheless, these cells introduce potential risks, including graft-versus-host disease and rejection by the recipient's immune system.
A common method to quantify T-cells, B-cells, and NK-cells in clinical trials involving CAR-T therapy is the standard 6-color (CD45, CD3, CD4, CD8, CD19, CD16/56) TBNK assay.
However, allogeneic CAR T-cells have their TCRαβ knocked out to mitigate the risk of a graft-versus-host reaction, resulting in a lack of surface CD3 expression. Consequently, in patients treated with allogeneic CAR T-cells, the CD3- compartment comprises not only CD19+ B cells and CD16+/56+ NK cells but also CAR T-cells.
An additional complication arises from the potential expression of CD56 on the surface of allogeneic CAR T cells due to activation. In such scenarios, utilizing the standard TBNK assay can lead to the erroneous categorization of CD16+/56+CD3- CAR T cells as NK-cells. To address this, the NK cell marker NKp46 was incorporated into the standard TBNK assay, and CD16 and CD56 were allocated to separate fluorochromes. This necessitated a panel redesign for optimal configuration and a modified gating strategy to accurately identify all cell populations, ensuring a clear distinction between host NK cells and CD56+CD3- CAR T cells. Within this gating strategy, NK cells are identified as CD45+CD3-CD4-CD8+/-CD56+CD16+/-NKp46+.
An optimized assay is presented here that mirrors the standard TBNK lyse/no-wash procedure in a BD Trucount™ tube to determine the absolute count of each population.
The newly developed assay underwent validation according to CLSI H62* guidelines to assess precision (repeatability and reproducibility), between-instrument variability, and between-operator variability. Sample stability for the optimized TBNK assay was established at 120 hours when samples were kept at ambient temperature. Furthermore, a successful experimental design is detailed that enabled the determination of lymphocyte detection sensitivity, with a lower limit of detection (LLoD) of 2 cells per μl and a lower limit of quantitation (LLoQ) of 6 cells per μl. Consequently, the optimized TBNK assay was validated for secondary endpoint use in clinical trials for allogeneic CAR T therapy.
*CLSI (Ed.). Validation of assays performed by flow cytometry,1st ed. CLSI document H62. Wayne,PA: Clinical Laboratory Standards Institute, (2021).
Panel configuration (BD FACSLyric™)
Source: Cerba Research
Detector
(laser) |
FL1
(405) |
FL2
(405) |
FL3
(405) |
FL4
(405) |
FL5
(405) |
FL6
(488) |
FL7
(488) |
FL8
(488) |
FL9
(488) |
FL10
(640) |
FL11
(640) |
FL12
(640) |
Fluorochrome
(Filter) |
BV421
(448/
45) |
BV510
(528/
45) |
BV605
(606/
36) |
BV711
(715/
50) |
BV785
(755
LP) |
FITC
(527/
32) |
PE
(586/
42) |
PerCP-Cy5.5
(700/54) |
RB780
(783/
56) |
APC
(660/
10) |
APC-
R700
(720/30) |
APC-
Cy7
(783/56) |
| Tube 1* |
|
|
CD45 |
|
CD8 |
CD4 |
CD19 |
CD20 |
CD16 |
NKp46 |
|
CD56 |
CD3 |
*Trucount tube; Lyse/No Wash
Optimization of gating strategy
Traditional gating leads to inclusion of CD56+CD3- allogeneic CAR T cells in the NK-cell population
The absence of CD3 expression in allogeneic CAR T cells presents a unique challenge in identifying NK cells when employing the standard gating strategy from the 6-color (CD45, CD3, CD4, CD8, CD19, CD16/56) TBNK assay.
In patients receiving allogeneic CAR T- cells, the CD3- compartment contains not only CD19+ B cells and CD16+/56+ NK cells but also CAR T-cells. An additional layer of complexity is the expression of CD56 on the surface of allogeneic CAR T cells due to activation. This was demonstrated by comparing a whole blood (WB) sample from a healthy volunteer with a WB sample from the same volunteer spiked with allogeneic CAR T cells.
As illustrated in the Figure below, the CAR T cells (shown in turquoise and identified as CD3-CD4+ or CD8+) exhibiting CD56 expression are contaminating the NK cell gate. Therefore, employing the traditional gating from the 6-color TBNK assay results in the erroneous inclusion of CD56+CD3- CAR T cells within the CD16/CD56+CD3- NK-cell compartment.
Healthy volunteer whole blood
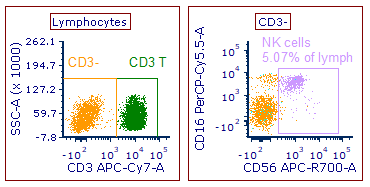
Image Credit: Cerba Research
Healthy volunteer whole blood spiked with allogeneic CAR T cells
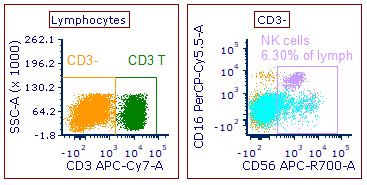
Image Credit: Cerba Research
The addition of the NK cell marker NKp46 allows for proper distinction of host NK cells from CD56+ CD3- CAR T cells
To enable accurate differentiation of host NK cells from CD56+CD3- allogeneic CAR T cells, the panel design was modified by incorporating the NK cell marker NKp46 and distributing CD16 and CD56 across two distinct fluorochromes. Subsequently, an optimized gating strategy was developed to isolate the NK cell gate from potential CD56+CD3- contaminating CAR T cells. In this refined gating strategy, B cells are now identified as CD19/CD20+ cells within the CD3-CD4-CD8- lymphocyte.
Furthermore, supplementary purification gates were introduced in the hierarchy to separate genuine NK cells from potential CD56+ allogeneic CAR T cells. Initially, CD56+ cells are selected within the CD3-CD4- lymphocytes, which effectively excludes CD4+ CAR T cells. At this stage of the gating hierarchy, it is not yet possible to exclude CD8+ CAR T cells, as a subset of NK cells can express CD8+. In the subsequent step, termed 'NK purification,' NK cells are further isolated from CD56+ CAR T cells using CD16 and the additional NK cell marker NKp46.
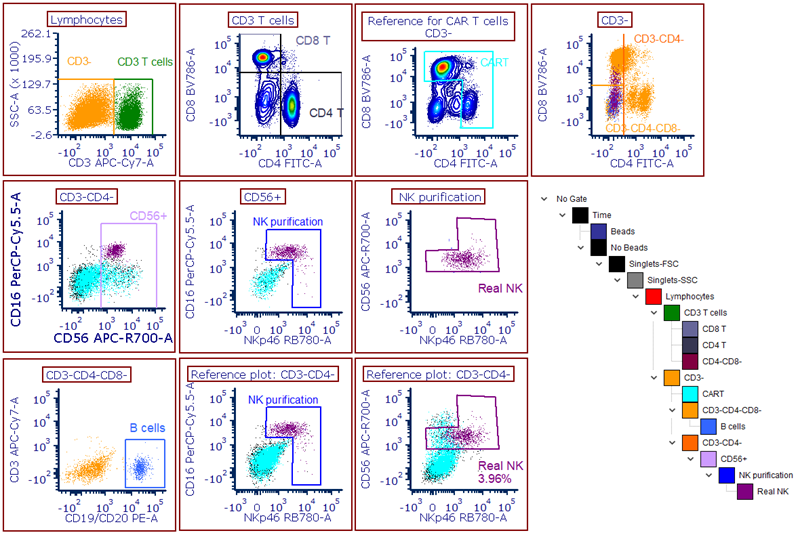
Image Credit: Cerba Research
Panel validation
Precision
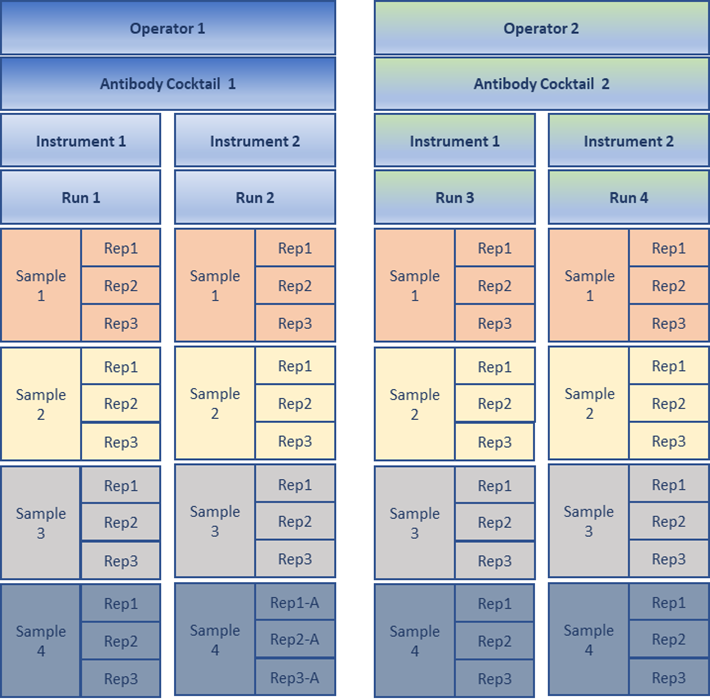
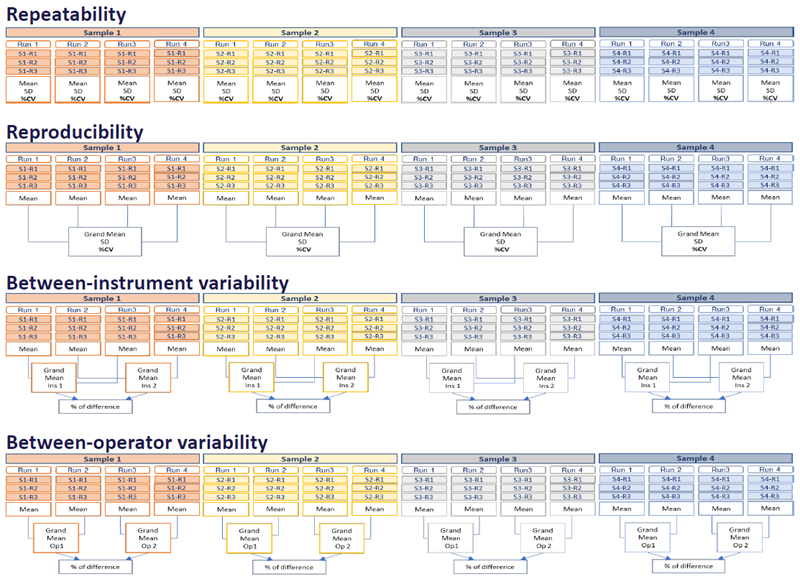
Precision was assessed using four WB samples from apparently healthy donors, with two of these donors being spiked with allogeneic CAR T cells. Samples were processed in triplicates by two operators and acquired on two instruments across a total of four distinct runs. For repeatability (intra-assay precision) and reproducibility (inter-assay precision), acceptance criteria of ≤ 25% CV between replicates/runs were applied. Higher imprecision (35% CV) was permissible for rare populations (≤ 5% of parent or ≤ 100 events) or populations with dimly expressed antigens. For between-instrument and between-operator variability, acceptance criteria of ≤ 20% difference between instruments/operators were applied.
| |
Repeatability |
Reproducibility |
Inter-instrument |
Inter-operator |
| Reportables |
%CV (average
of 4 samples) |
%CV (range over
4 samples) |
% difference
(range over
4 samples) |
% difference
(range over
4 samples) |
| Lymphocytes |
2.85 |
0.90 - 6.50 |
0.11 - 2.66 |
1.06 -11.07 |
| T cells (% of Lymph) |
0.70 |
1.21 - 2.15 |
0.05 - 3.06 |
0.30 -2.06 |
| T cells (abs.) |
2.86 |
1.93 - 5.90 |
1.05 - 3.03 |
1.35 -9.30 |
| CD4 T cells (% of Lymph) |
1.10 |
1.20 - 2.00 |
0.03 - 3.03 |
0.06 -1.48 |
| CD4 T cells (% of T cells) |
0.70 |
0.13 - 0.62 |
0.03 - 0.58 |
0.02 -0.38 |
| CD4 T cells (abs.) |
2.95 |
1.55 - 6.12 |
1.15 - 3.04 |
1.13 -9.73 |
| CD8 T cells (% of Lymph) |
1.26 |
1.31 - 3.25 |
0.60 - 3.32 |
0.24 -4.56 |
| CD8 T cells (% of T cells) |
0.74 |
0.57 - 2.57 |
0.11 - 0.63 |
0.86 -4.25 |
| CD8 T cells (abs.) |
3.22 |
1.51 - 4.89 |
0.45 - 3.25 |
1.58 -7.19 |
| B cells (% of Lymph) |
1.44 |
0.99 - 2.48 |
0.05 - 4.00 |
0.64 -1.54 |
| B cells (abs.) |
3.17 |
1.45 - 6.22 |
1.16 - 4.01 |
0.73 -9.70 |
| NK cells (% of Lymph) |
2.45 |
2.57 - 10.88 |
0.00 - 4.88 |
4.13 -13.30 |
| NK cells (abs.) |
4.34 |
4.17 - 11.42 |
0.92 - 3.91 |
6.67 -14.53 |
All reportables met the acceptance criteria for repeatability, reproducibility, between-instrument variability, and between-operator variability. Noticeably, precision of all reportables is below 12% CV and between-instrument and between-operator is less than 15% difference for all reportables, indicating a highly robust assay. Image Credit: Cerba Research
Sample stability and post-stain stability
Sample stability was evaluated on six WB samples from apparently healthy donors, processed at baseline (within 2 hours post-collection) and at 24, 48, 72, 96, and 120 hours from collection time. Between time points, samples were stored at ambient temperature (18-26 °C). Post-stain stability was determined on six WB samples from apparently healthy donors, acquired at baseline (within 30 minutes after staining), and at 1, 3, and 24 hours from baseline. Stained samples were kept at ambient temperature for up to 3 hours post-baseline and subsequently refrigerated (2-6 °C) for 24 hours.
Sample stability and post-stain stability were both established at the latest time point where a change of ≤ 20% from baseline was achieved for at least 80% (5 out of 6) of the samples. Results indicated that samples remain stable for up to 120 hours post-collection for all reportable analytes. However, for NK cells, a decline in signal was observed for NKp46, and to a lesser extent for CD16 and CD56, over time. Nevertheless, the gating strategy utilizing all three markers, along with the panel design with CD56 and CD16 distributed across two fluorochromes, still permits accurate identification of the NK cell population. Post-stain stability was confirmed up to 3 hours after staining when stored at room temperature, and up to 24 hours after processing when stored refrigerated.
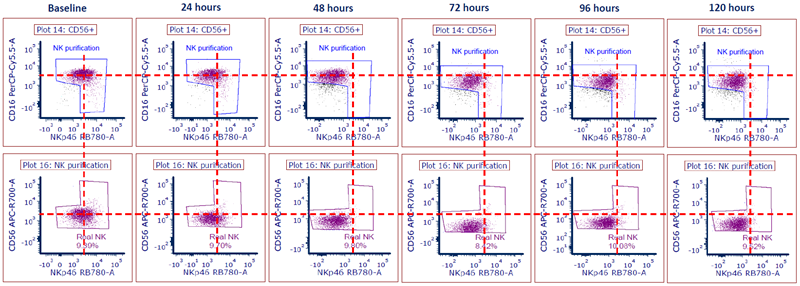
Image Credit: Cerba Research
Sensitivity – Lower limit of detection (LLoD) and lower limit of quantitation (LLoQ) assessment for lymphocytes absolute count significant
Severe lymphodepletion is a prerequisite for treatment with allogeneic CAR T cells to minimize the risk of host-versus-graft disease. Therefore, determining the LLoD and LLoQ for the absolute lymphocyte count of the optimized TBNK assay is essential. The LLoD for lymphocytes absolute count was established using two whole blood samples from apparently healthy donors in a total of 10 CD45-negative runs, as depicted in the experimental setup below. Subsequently, the LLoD was calculated using the formula: LLoD = Mean + 3 SD. The results revealed an LLoD of 2 cells/μl for lymphocytes absolute count.
Source: Cerba Research
| Experimental setup |
Sample 1 |
Sample 2 |
| Processing |
CD45 FMO* |
CD45 FMO* |
| Acquisition |
5 x per tube = 5 runs |
5 x per tube = 5 runs |
*Stained with all antibodies except CD45 (FMO)
Source: Cerba Research
| Results |
Mean (cells/μl) |
SD (cells/μl) |
LLoD (cells/μl) |
| Lymphocytes (abs.) |
0.60 |
0.52 |
2.15 |
LLoQ for lymphocytes absolute count was determined using three whole blood samples from apparently healthy donors. Each sample underwent duplicate processing: one with the standard full stain (FS) antibody cocktail and another with an unlabeled CD45 antibody (without other antibodies). Subsequently, five different serial dilution levels were created in triplicate, as illustrated in the example below. For each sample and dilution, the mean, SD, and %CV were calculated for lymphocytes absolute count. The LLoQ was established at the level where a ≤ 35% CV was achieved in at least 2 out of 3 samples, provided a minimum of 50 events were present within the population gate and all triplicates exceeded the LLoD. Based on all three samples, the LLoQ for lymphocytes absolute count was determined to be 6 cells/μl.
Source: Cerba Research
Experimental setup
for 1 sample |
Processed with CD45
unlabeled antibody |
Serial
dilution |
Dilution
factor |
| Tube 1 |
458 μl |
42 μl stained with
FS cocktail |
12 |
| Tube 2 |
375 μl |
125 μl from tube 1 |
48 |
| Tube 3 |
375 μl |
125 μl from tube 2 |
192 |
| Tube 4 |
375 μl |
125 μl from tube 3 |
768 |
| Tube 5 |
375 μl |
125 μl from tube 4 |
3072 |
Source: Cerba Research
| Results |
Sample 1 |
Sample 2 |
Sample 3 |
| Dilution |
Mean |
SD |
%CV |
Mean |
SD |
%CV |
Mean |
SD |
%CV |
| 1:12 |
100.67 |
3.51 |
3.49 |
95.00 |
8.54 |
8.99 |
106.00 |
3.00 |
2.83 |
| 1:48 |
35.00 |
1.00 |
2.86 |
22.00 |
3.00 |
13.64 |
23.33 |
1.53 |
6.55 |
| 1:192 |
8.33 |
0.58 |
6.93 |
5.67 |
0.58 |
10.19 |
6.00 |
0.00 |
0.00 |
| 1:768 |
2.67 |
0.58 |
21.65 |
1.33 |
0.58 |
43.30 |
1.33 |
0.58 |
43.30 |
| 1:3072 |
0.67 |
0.58 |
86.60 |
0.00 |
0.00 |
UC |
0.33 |
0.58 |
173.21 |
Table Legend. Source: Cerba Research
| |
| Pass (< 35% CV) |
| Fail (> 35% CV) |
| Unable to calculate (UC) |
| Used for LLoQ |
| Below LLoD (< 2 cells/μl) |
Conclusion
The data presented in this poster underscore the capability of the optimized TBNK assay to accurately identify NK-cells from CD56+ allogeneic CAR T cells. Furthermore, it was demonstrated that the assay was validated according to CLSI H62 guidelines for use as a secondary endpoint in clinical trials. A sample stability of 120 hours and post-stain stability of 24 hours were established, allowing for testing at central laboratories within an extended timeframe. Finally, the assay exhibited high sensitivity, with an LLoD of 2 cells/μl and an LLoQ of 6 cells/μl for CD45+ lymphocytes.
About Cerba Research
Mission
Cerba Research provides innovative laboratory solutions for clinical research to support their customers in bringing improved treatments to patients.
Vision
To be the world leading, specialty laboratory solution provider in clinical research, supporting their customers with faster diagnosis, development, and delivery of patient treatments.
Company profile
Cerba Research is a leading specialty laboratory services provider with the capacity and breadth of a global central laboratory network. Their highly qualified scientists provide insight on the latest biomarkers, assays and testing approaches and develop innovative solutions for unique challenges across all research phases, to pharmaceutical, biotechnology, medical device, government, public health, and CRO organizations.
Cerba Research’s extensive capability in laboratory testing and global logistics including Bioanalysis, Flow Cytometry, HistoCytopathology, and Next-Generation Sequencing, enables them to drive operational agility at scale in a wide range of therapeutic areas, with recognized expertise in Virology, Immunology, Oncology and Cell & Gene Therapy.
Cerba Research is part of the Cerba HealthCare Group with 15,000 employees on five continents, driven to advance diagnosis and health.
For more information about Cerba Research, please visit cerbaresearch.com.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.net, which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.
Last Updated: Jun 25, 2026
 Cerba Research Expands U.S. Immuno-Oncology Center of Excellence to Strengthen Its Precision Medicine Offerings
Cerba Research Expands U.S. Immuno-Oncology Center of Excellence to Strengthen Its Precision Medicine Offerings