This article is based on a poster originally authored by Joel A. Meyboom, Sjoerd C. Ingelse, Ilse H. Wolters, and Karthikeyan Devaraju.
Chimeric antigen receptor T-cell (CAR-T) therapies are considered essential for both oncology and autoimmune disease applications. CAR T-cells and other CAR-immune cells, in addition to TCR-T therapies, are predominantly created through the process of lentiviral/retroviral vector transduction.
During CAR-T therapies, it is absolutely necessary to monitor patient safety and pharmacokinetic efficacy.1 Safety monitoring is conducted by testing for replication-competent lentivirus/retrovirus (RCL/R) with qPCR, and pharmacokinetics is evaluated by testing for vector copy numbers (VCN) with ddPCR. Genomic DNA must be isolated from a patient’s whole-blood (WB) sample when running the RCL/R and VCN assays.
Prior to CAR T-cell infusion, patients must be lymphodepleted, whether for autologous or allogeneic therapy. Lymphodepletion typically results in patients having very few or no lymphocytes in their blood during the first few days of CAR-T therapy.
Lymphocytes are crucial for monitoring RCL/R and VCN at specific intervals before and after CAR T-cell infusion. VCN is carried out from day (d) 0 to day 28 of CAR therapy at predetermined times. During this phase, there are a limited number of lymphocytes (DNA) available before recovering the lymphocytes, including the CAR T-cells, in the patient.
To ensure there is sufficient DNA available during the first two weeks of CAR monitoring, DNA should be pulled using as much sample input volume as possible. This means that any automated extraction procedure faces a significant challenge, which also affects the efficiency of downstream molecular assays.
Objectives
- Isolation of DNA sufficient for VCN and RCL/R testing from patients experiencing CAR/TCR-T-cell therapies, while running an automated nucleic acid isolation platform
- Validation of the nucleic acid isolation process for clinical samples
Materials and methods
Peripheral venous blood (WB) samples were acquired from healthy volunteers and taken after informed consent. Nucleic acid isolation (NAI) was conducted using two different automated platforms.
Isolated DNA concentrations were determined by a Qubit (v4.0, ThermoScientific) fluorometer, while the quality of the isolated DNA was assessed by agarose gel electrophoresis.

Image Credit: Cerba Research
Results
1. Improving DNA yield
-
- It was found that increasing the volume of WB input did not increase DNA yield (Figure 1).
- Different workflows were tested to maximize the isolated DNA yield.
- A workflow was determined using the automated platform that generated improved yields of DNA (Figure 2).
2. Validating the automated isolation workflow
-
- Subsequently, the optimized workflow was validated with two different operators (Op1 and Op2) with multiple samples on different days.2
- The results exhibited how the DNA yield could be scaled alongside the volume of sample input (Figure 2).
- The isolated DNA was validated in line with the RCL and VCN assays using spike-in controls.2,3 All control samples with a spike-in were tested positive with a CV% <20% for the RCL assay (qPCR) and for ddPCR: CV <20% for >50 copies/PCR and a CV <40% for copies <50 copies/PCR. Control DNA samples without spike-in controls showed as negative.
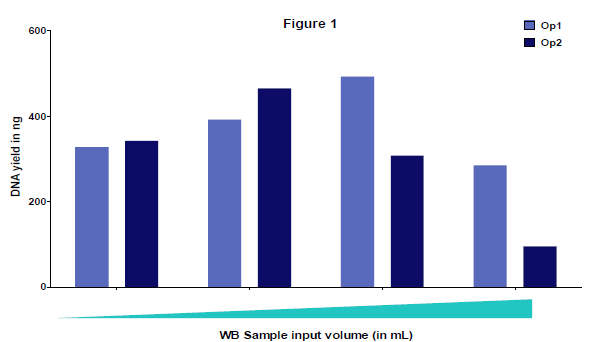
Figure 1. Verification results to determine if increasing volume of WB sample input (from 0.5–4 mL) improves DNA yield. Isolation was performed by two different operators (Op1 and Op2). Isolated DNA yield did not improve with increasing sample input volume. The variation between the operators was due to the biological nature of the samples. Image Credit: Cerba Research
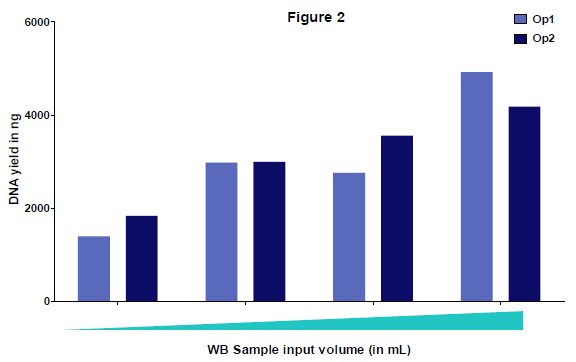
Figure 2. Validation results: optimized workflow for different volumes of WB sample input (from 0.5–4 mL). Isolation was performed by two different operators (Op1 and Op2). Isolated DNA yield improved with increasing sample volume. Results show that DNA yield was scalable or linear with the volume of sample input. The variation between the operators was due to the biological nature of the samples. Image Credit: Cerba Research
Conclusion
- The researchers demonstrate how a scalable workflow was optimized and validated for the automated isolation of DNA from WB samples, maximizing DNA yield per sample.
- The DNA yield and quality obtained are deemed appropriate for safety monitoring testing (qPCR and ddPCR) in CAR-T clinical trial patient samples.
- The next steps will explore the optimized workflow for total nucleic acid isolation, for both DNA and RNA.
References and further reading:
- FDA (2024). Considerations for the Development of Chimeric Antigen Receptor (CAR) T Cell Products. U.S. Food and Drug Administration. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-development-chimeric-antigen-receptor-car-t-cell-products.
- FDA (2018). Research, C. for D.E. and (2020). Bioanalytical Method Validation Guidance for Industry. U.S. Food and Drug Administration. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry.
- ISO (2019). Biotechnology - Requirements of evaluating the performance of quantification methods for nucleic acid target sequences - qPCR and dPCR. ISO. Available at: https://www.iso.org/standard/67893.html?__cf_chl_f_tk=z3UM_3ySTHwaQ17iWmSCc8j38MtZFh4OD.HZR8cZAAs-1783049562-1.0.1.1-GGMtZZ5zS.XDbqOsMQ5VQ5SfOH_tMbuLDbtrgOYGTtQ.
About Cerba Research

Cerba Research is a leading specialty laboratory services provider with the capacity and breadth of a global central laboratory network. Their highly qualified scientists provide insight on the latest biomarkers, assays and testing approaches and develop innovative solutions for unique challenges across all research phases, to pharmaceutical, biotechnology, medical device, government, public health, and CRO organizations.
Cerba Research’s extensive capability in laboratory testing and global logistics including Bioanalysis, Flow Cytometry, Histopathology, and Next-Generation Sequencing, enables them to drive operational agility at scale in a wide range of therapeutic areas, with recognized expertise in Virology, Immunology, Oncology and Cell & Gene Therapy.
Cerba Research is part of the Cerba HealthCare Group with 15,000 employees on five continents, driven to advance diagnosis and health.
For more information about Cerba Research, please visit cerbaresearch.com.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.net, which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.
Last Updated: Jul 8, 2026
 Cerba Healthcare to acquire Canadian contract research laboratory Cirion Biopharma Research to expand bioanalytical capabilities and shorten time-to-deploy complex clinical trials
Cerba Healthcare to acquire Canadian contract research laboratory Cirion Biopharma Research to expand bioanalytical capabilities and shorten time-to-deploy complex clinical trials