This article is based on a poster originally authored by Rania Gaspo, Renaud Burrer, Jérôme Sallette, Amanda Finan-Marchi, and Marie Gérus-Durand.
NSCLC (non-small cell lung cancer) treatment is seeing advances that increasingly depend on precise biomarker-driven strategies, with targeted therapies offering clear advantages over cytotoxic agents.
However, the rapid increase of rare, actionable biomarkers makes routine detection and integration into clinical practice particularly challenging. Therefore, to ensure each patient receives timely and appropriate therapy selection, accurate and efficient biomarker characterization is crucial.
Introduction
Annually, over 1.8 million deaths are caused by lung cancer, with around 85% of cases being represented by NSCLC.1,2 This cancer is extremely diverse at the genetic level, so tools such as next-generation sequencing (NGS) panels and immunohistochemistry (IHC) are critical for comprehensive biomarker testing that guides optimal treatment strategies.
To define which biomarkers and assays can be used, international guidelines (CAP, IASLC, AMP, ASCO, NCCN, and the Canadian consensus) have been established.3
Table 1. Druggable and exploratory targets with pre-identified antibodies to be tested through simplex IHC on NSCLC formalin-fixed, paraffin-embedded (FFPE). Source: Cerba Research
| Target |
Selected Rx* |
Antibody Clone |
Expected Positivity Rate |
| ALK |
Crizotinib, Ceritinib, Alectinib, Brigatinib, Lorlatinib |
D5F3 |
3%4-5 |
| ROS1 (+/- FISH) |
Crizotinib, Lorlatinib, Entrectinib |
SP364 |
1–2%4-6 |
| HER2 |
Trastuzumab, Pertuzumab |
DG44 |
1–5% |
| EGFR |
Erlotinib, Gefitinib, Dacomitinib, Osimertinib |
3C6 |
10–15%4-5 |
| Pan-TRK |
Larotrectinib, Entrectinib |
EPR17341 |
< 1%6 |
| BRAF |
Vemurafenib, Dabrafenib |
VE1 |
4%4-5 |
| cMet |
Crizotinib, Tivantinib, Onartuzumab |
SP44 |
3-4%7 |
| MEK1 |
Trametinib, Binimetinib, Selumetinib |
H-8 |
/ |
*Selected treatments that target the specific biomarker.
Method and workflow

Image Credit: Cerba Research
Results
IHC data concordance study with genetic profiling and observed prevalence
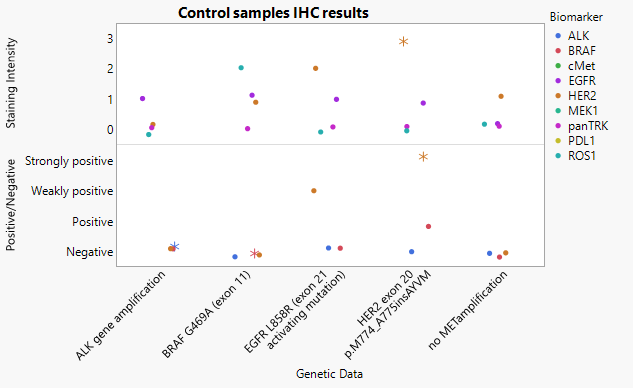
Figure 1. IHC staining results for tissue controls. Image Credit: Cerba Research
* Indicates slides for which the pathologist made a comment
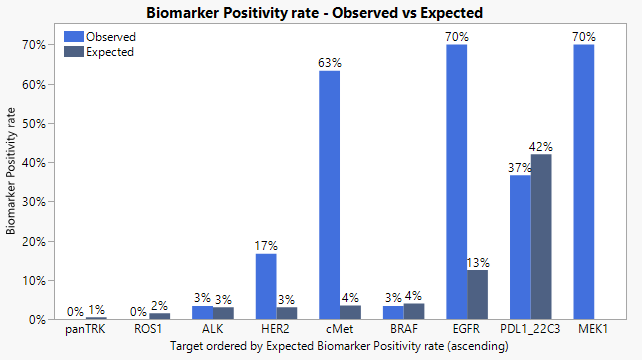
Figure 2. Biomarker positivity rates in tested samples. Image Credit: Cerba Research
IHC performance on control samples (Figure 1) exhibited strong correlation with NGS for HER2, cMET, and EGFR. This demonstrates the reliability of the IHC panel across these targets.
Compared to the other controls, HER2 expression was considerably more intense. The pathologist noted that BRAF exhibited no IHC staining, consistent with a non-V600E mutation and supporting assay specificity regardless of an atypical pattern (weak cytoplasmic/moderate nuclear signal).
For ALK, NGS did not detect strong protein expression in the gene amplification. However, focal IHC positivity led to an advisory for reflex fluorescence in situ hybridization (FISH)/NGS, highlighting the role IHC plays as an appropriate screening step for ALK alterations.
Across the 25 unknown samples, an alignment was observed in biomarker positivity rates (Figure 2) correlating with the published NSCLC prevalence. There was a fall in ALK, BRAF, and PD-L1 frequencies, which were in the expected ranges, while EGFR and cMet were moderately higher, further endorsing the use of IHC for rapid upfront stratification before molecular testing.
No positive ROS1 cases were identified, and the same results were tracked for pan-TRK, which is consistent with their low occurrence in NSCLC. Together, the data underscores how IHC can act as a powerful first-line approach for identifying principal NSCLC biomarkers to support efficient reflex FISH/NGS testing.
Evaluating biomarker relationships
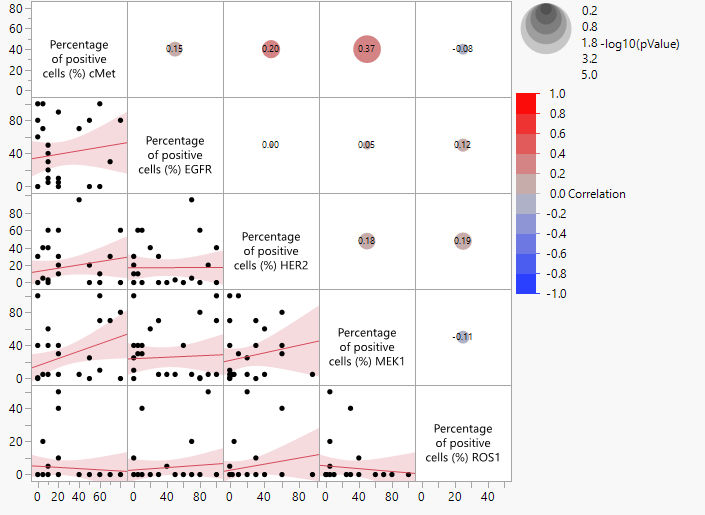
Figure 3. Scatter plot Matrix showing correlations in IHC percentages of positive cells among tested biomarkers. panTRK results were omitted because no sample was positive for this marker. Image Credit: Cerba Research
Across all 30 NSCLC samples supplied by Cerba Research Biobank, IHC displayed heterogeneous biomarker expression. Pan-TRK, BRAF, ALK, and ROS1 exhibited extremely low levels of staining, which is not conducive to reliable interpretation.
Although some samples were able to achieve 50% focal staining, the criteria for true positivity were not met, as no diffuse 2+/3+ ROS1-like patterns were observed by the international pathologist. Figure 3 shows both the distribution of detectable biomarkers and the low prevalence of rare targets, and reveals how IHC-based biomarker matrices can aid in more accurate treatment strategies for patients.
Samples’ biomarker signature
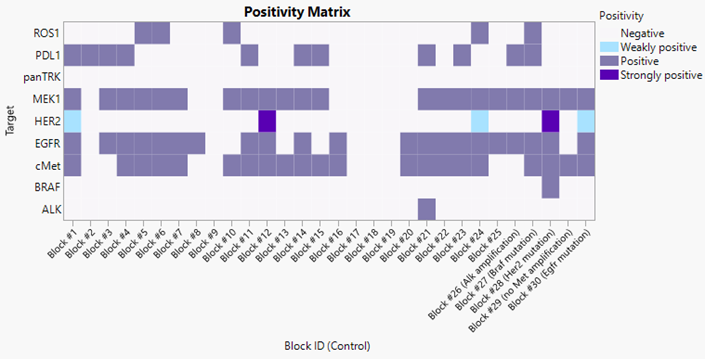
Fig 4. Positivity matrix showing biomarker positivity for each tested sample. Image Credit: Cerba Research
The scatter plot matrix exhibited clear patterns of co-occurrence across the biomarkers tested. The greatest correlation was seen between cMet and MEK1, with 37% of samples exhibiting concurrent expression. This indicates a potential linkage in signaling pathways or shared regulatory mechanisms.
Similarly, a significant trend was observed between cMet and HER2, which co-occurred in 20% of cases, suggesting that these changes may cluster within a subset of NSCLC tumors. These relationships underscore how IHC-based profiling can be a powerful tool for uncovering biomarker patterns that may aid both diagnostic interpretation and future molecular testing strategies.
Conclusion
IHC demonstrated exceptional reliability in identifying key biomarkers across control and unknown NSCLC samples and exhibited a high correlation with NGS for HER2, cMet, and EGFR. The panel successfully identified positivity rates as expected across the 25-sample cohort, with ALK, BRAF, and PD-L1 matching with known prevalence.
Moreover, EGFR/MEK1 appeared slightly higher, which supports the idea that IHC acts as a rapid first-line screening method prior to reflex molecular testing.
Rare targets, including BRAF, ROS1, ALK, and pan-TRK, demonstrated minimal or non-interpretable staining, consistent with their low prevalence in NSCLC. Visualization tools such as scatter plot matrices and heat maps reveal heterogeneous biomarker expression and significant co-occurrence patterns, especially between cMet, MEK1, and HER2.
Together, these findings indicate that IHC delivers a powerful, efficient approach for early NSCLC biomarker stratification while supporting identification of clinically relevant expression patterns. This aids timely and relevant downstream testing and treatment selection.
IHC can be considered a robust and accessible screening method for the majority of actionable biomarkers, especially when routine NGS is not available. This means IHC pathology workflows can lead to the optimization of patient selection for precision medicine and clinical trial enrolment.
References and further reading
- About lung cancer. American Cancer Society;
- World Health Organization (2023). Lung Cancer. World Health Organization. Available at: https://www.who.int/news-room/fact-sheets/detail/lung-cancer.
- National Comprehensive Cancer Network (2025). National Comprehensive Cancer Network. National Comprehensive Cancer Network. Available at: https://www.nccn.org/.
- American Lung Association (2023). American Lung Association. American Lung Association. Available at: https://www.lung.org/.
- American Cancer Association;
- Facchinetti, F., et al. (2017). Oncogene addiction in non-small cell lung cancer: Focus on ROS1 inhibition. Cancer Treatment Reviews, 55, pp.83–95. doi:https://doi.org/10.1016/j.ctrv.2017.02.010. https://www.cancertreatmentreviews.com/article/S0305-7372(17)30029-4/abstract.
- Cancer Support Community (2024). Cancer Support Community. Cancer Support Community. Available at: https://www.cancersupportcommunity.org/.
About Cerba Research

Cerba Research is a leading specialty laboratory services provider with the capacity and breadth of a global central laboratory network. Their highly qualified scientists provide insight on the latest biomarkers, assays and testing approaches and develop innovative solutions for unique challenges across all research phases, to pharmaceutical, biotechnology, medical device, government, public health, and CRO organizations.
Cerba Research’s extensive capability in laboratory testing and global logistics including Bioanalysis, Flow Cytometry, Histopathology, and Next-Generation Sequencing, enables them to drive operational agility at scale in a wide range of therapeutic areas, with recognized expertise in Virology, Immunology, Oncology and Cell & Gene Therapy.
Cerba Research is part of the Cerba HealthCare Group with 15,000 employees on five continents, driven to advance diagnosis and health.
For more information about Cerba Research, please visit cerbaresearch.com.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.net, which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.
Last Updated: Jul 8, 2026
 The critical role of flow cytometry in CAR+ T-Cell trials
The critical role of flow cytometry in CAR+ T-Cell trials