The survey showed that only 50% of women consulted a healthcare professional about their symptoms, despite the fact that many women said their symptoms were having a significant effect on their work life, social life, home life and sex life.
In our survey, about 35% of women said the menopause significantly affected their work. It affected their functioning, their performance and their confidence.
If women aren't having significant symptoms that are too troublesome, then it’s okay if they don't need to seek help. However, it's not just the fact that 50% weren't seeking help, it's about the number of women that were having symptoms that were affecting them, but seemingly not doing anything about it.
What is the Menopause?
Did the survey go into the reasons why these women weren't seeking help?
It did. Some of the women didn't think the symptoms were bad enough and some of them felt they just had to put up with it and just accepted it as a normal stage of life.
Some women felt that if they did go to see the GP, all that would happen would be that they would be offered hormone replacement therapy (HRT) and a lot of women expressed a concern about the use of HRT.
Were you surprised by these results?
Given the NICE guidelines for menopause were published in November and generated a lot of media coverage in the UK, we’d hoped to see more women stating they were seeking help and recognising the support and information out there for them, but the survey highlighted the scale of the educational challenge that remains to ensure women aren’t suffering in silence.
Can you please give an overview of the recently published NICE guideline on the diagnosis and management of the menopause?
It has various sections. The first is about the importance of women getting information. There is awareness that women and healthcare professionals have been given very mixed messages over the years, whether it's from research studies or media reporting. There's been a lot of confusion about the effects of the menopause and how long effects can last for, as well as about the benefits and risks of various treatments.
Women should have access to accurate information, which is why we've developed websites and updated resources, including online resources. We’ve provided a lot of tools to help women get the right information.

The next thing is emphasizing the importance of individualization, since no two women are the same. How the menopause affects women and what the rules are for different dietary and lifestyle changes or treatments, is very individual. Also, even within one woman, it's important to know that the stages of menopause and how menopause is affecting her can change over the years, which then also has an effect on her treatment needs.
Regarding diagnosis of menopause, the simple message is that for women aged over 45 who have menopausal symptoms such as a change in periods or absent periods, we don't need to do a blood test. In the past, blood tests had often been taken to measure hormone levels and we feel that for many women, that's not necessary. As well as the cost of the blood test, there's also the need for another consultation to discuss the results, which means there is often a delay in starting management because they're waiting for the results. The practical thing is to do less blood tests to diagnose menopause.
There is advice about women being aware of the recommendations on diet and lifestyle changes, both to reduce their early symptoms and also to improve their long-term health. Information is needed to help women understand the different stages of going through the perimenopause and the menopause, the range of symptoms which may occur and what treatment options are available.
For treatment of symptoms such as hot flushes, night sweats, and low mood the recommendation is to offer HRT. For the majority of women, the benefits of HRT outweigh the risks.
There are also some specifics about the benefits and risks of long term treatment, but for the early symptoms, the clear message is to offer HRT. At the moment, there are a lot of women experiencing symptoms that are having a big impact on their lives and who could benefit from treatment, but they accessing treatment because of perceived risks of HRT.
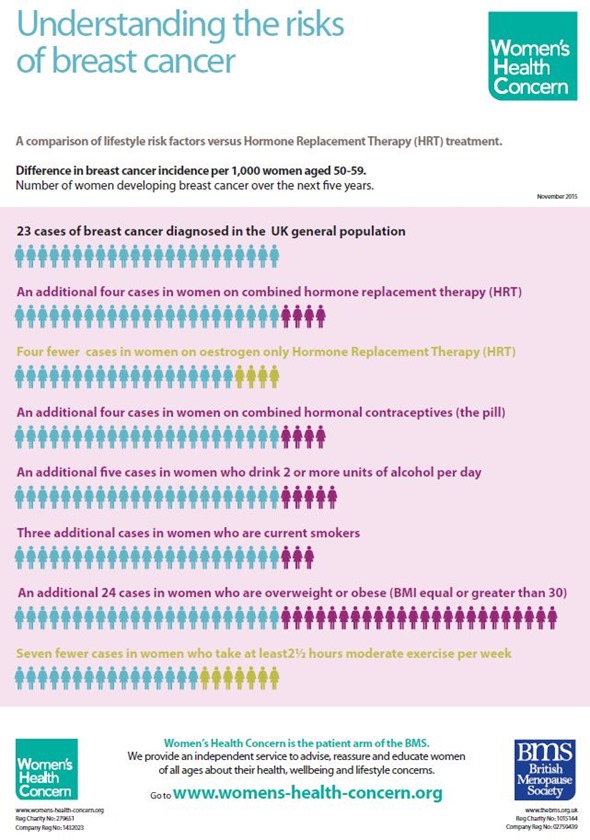
One of the resources we've developed is an infogram about perceived risks and also the big thing that women worry about, which is the risk of breast cancer. We've compiled a really helpful chart, which shows the numbers of women and the estimated expectation of association of breast cancer with HRT, as well as its association with drinking alcohol, and particularly obesity, which is a far bigger risk factor than the use of HRT. The message regarding breast cancer is that HRT doesn't cause cancer, but may promote the growth of cancer cells that are already present in some women.
Regarding the duration of treatment another message is that there's no arbitrary limit. Often, in the past, if women have taken HRT, they've been told they would have to stop it at a certain time. Actually, it's up to the woman. If she's taking it for symptoms, you can never predict how long the symptoms will go on for, so you can't predict how long treatment will be needed for.
The British Menopause Society website is for health professionals, but we've added in the top ten messages in order to summarise the NICE guideline and help people access the information.
Do you think these guidelines will encourage more women to seek help?
The first thing is for more women to get information. However, there is a concern that primary care in the UK is under huge pressure, so we don't want people to think we're encouraging lots more women to go to their GP and that GPs will be even more inundated.
The point is that if women get access to information using, for example, the various resources we have to help them, then, if they do go to their healthcare professional, they can have a much more useful discussion. You can't cover all of the information that's required in a short appointment, so, inevitably, that might lead to another appointment. However, if women can already be informed when they go, then they can have a more informed discussion, which can be really useful.
Once women have got the information, it may be that some of them are actually able to make diet and lifestyle changes and that might be all that's required. However, if they do require treatment, then they would need to go to a healthcare professional to have that prescribed or they may want to have a further discussion. Either way, it would be useful for them to have some information first.
Effects of the Menopause
In what ways do you plan to raise awareness of the NICE guideline?
The launch of the campaign in May was the first part of raising awareness and we want to continue providing education. We provide education for healthcare professionals through the British Menopause Society. We have a whole program of meetings planned and a publication that goes out to all our members.
For women, the campaign received a lot of media attention. That was great, but we also have some things coming out in long lead publications, so we have other menopause stories that will be coming out over the next few weeks and few months or so. We hope that the use of our websites and the range of websites will increase. We're also using social media, just to keep the message going. It's a case of sort of drip feeding the message really, to keep the awareness up; not just awareness of the NICE guideline, but awareness of the importance of menopause.
What misconceptions do people have about the menopause?
First of all, I think many women focus on the symptoms that they expect and that the majority of women do have, which are flushes and sweats. One misconception is that it's just about flushes and sweats and what we're trying to educate people about is that the menopause is all about a lack of estrogen. Women’s bodies become low on estrogen because, in the majority of cases, our ovaries stop working. In a few women, the ovaries might be removed or might be affected by another treatment, but whatever type of menopause it is, it’s all related to the lack of estrogen.
What our survey reinforced is that there are often symptoms that women are not expecting such as low mood, disturbed sleep and joint aches, even though these are also really common. We are trying to get people to understand the other effects of estrogen deficiency. Also, because we're living longer, we're going to live longer with the consequences of estrogen deficiency.
When people are focusing just on flushes and sweats, they don’t understand the later effects. Women will often experience vaginal dryness and discomfort and bladder problems such as urinary infections and going to the loo more often or more urgently and all these things can be related to lack of estrogen. The lack of estrogen also affects our bone and heart health. Therefore, the misconception that it's just about flushes and sweats, means we're missing all this other important information.
I think the other misconception is that the early symptoms only last a short time, so we've seen a lot of women who just put up with it thinking, "Oh, this is going to go. It's not going to last that long." However, we now know that for many women, these symptoms that start early can last a long time. Those early symptoms do resolve in a lot of cases, but we do know women in their 70s and 80s who still have them.
Also, among women whose symptoms do resolve, they then think, "That's it, I'm through the menopause now." If you just focus on the periods stopping, flushes and sweats, you then don't have that understanding that the body is changing, as well as our bone and heart health and that we therefore do need to stop smoking, increase exercise and lose weight, if applicable, in order to also improve long-term health.
There isn't really such a thing as, "I'm through the menopause now." It really is about thinking, "Okay, I've stopped having flushes, but my body's still low on estrogen. What else can I do to help that?"
Regarding treatments, the big misconception is that HRT is risky and dangerous, when in fact, for the majority of women, there are more benefits than risks.
Hormone Replacement Therapy (HRT)
What are the benefits and risks of HRT?
The big benefit is that it is still the most effective treatment for controlling symptoms that arise due to estrogen deficiency. We know it is good for bone health, and that if HRT is taken, it can reduce the risk of osteoporosis and osteoporotic fractures. Although it didn’t come from the NICE guideline, another point is that there is more evidence suggesting that there may be a benefit on heart health if HRT is started early in the menopausal stage.
We used to believe that 15 years ago and women often took HRT for that benefit, even if they didn't have the symptoms. However, a publication that changed that view on HRT was an American trial that was published in 2002. Since then, it has been reanalyzed many times and people have returned to thinking that HRT in the early years is probably protective against heart disease. It had been seen as a risk, but, in fact, it is probably more likely to be a benefit.
There is an established, very small increased risk of having a deep vein thrombosis or a blood clot when taking the tablet form of HRT, so for women with risk factors for those, such as being overweight, we would recommend using estrogen that is absorbed through the skin, which is either in the form of a patch or a gel. Administration by that route doesn't have the same effect on our clotting system.
Then, the big concern is the breast cancer risk. The current understanding is that HRT doesn't cause breast cells to turn into cancer, but that certain types of HRT may promote the growth of cancer cells that are already there if it is taken for more than five years after the age of 50.
The important point here is that we have to individualize. All women will have an individual baseline risk of breast cancer; two women will have very different risks of developing breast cancer. It is a myth that HRT causes the cancer. It may promote the growth of cancer cells already present by a small count in some women. However, it's certain types of HRT and, against that, are the benefits we've described.
What more needs to be done to educate women about the information and support available?
We want to get the word out there as much as possible. There was a lot of press interest in May, which was fantastic and some more since then, so it's carrying on. There are radio programme opportunities and I was on one of our television programs recently, which was great.
We have various avenues for using social media. We're just trying lots of different ways to get the message out to women. There are the websites I've mentioned and I also publish a magazine called Menopause Matters.
We're happy to work with patient organizations. Since last week, we've already heard of a couple of people who are wanting to run group sessions for women, which we're also happy to help with. We help in any way we can really.
What do you think the future holds for managing menopause symptoms?
I think HRT has a lot of benefits. Not every woman would be advised to take HRT. For many women, simple things like diet and lifestyle changes can actually make a big difference, but for those who want specific treatments, I think we still have a lot of myths about risk to dispel and that we need to give women accurate information so they can make informed choices. At the moment, a lot of women are still making decisions based on old information or these myths that I have mentioned.
Since we know the consequences related to estrogen deficiency, it makes sense to have a very useful treatment that is going to put the estrogen back and replace what our bodies have stopped producing. We know there are lots of benefits. We know that it's not perfect; I don't think any medication is perfect, but now there is research looking at how we can maximize the benefits and absolutely minimize the risks.
The risks are already very small, but there is more interest in different ways of replacing the estrogen in as safe a way as possible. We need more scientific research on this, but we do have new preparations that will hopefully start to appear.
Diet and lifestyle are hugely important. There are some alternatives that may be helpful, so perhaps we need more research on those. There has been a concern about standardization of products and the products that we buy over the counter not being regulated in the same way as prescribed medicines. We could do with more information about those preparations, so that we are able to trust what's in them. We still need more research.
What’s your vision for the British Menopause Society?
The British Menopause Society's aim is to support and educate healthcare professionals. In the UK, the majority of care is given in primary care, so within primary care, we would love there to be a general basic understanding of the menopause and treatment options, which the NICE guideline has given us.
We just need to continue to provide simple versions of that. The full document is huge and busy GPs and practice nurses are unlikely to read it, so we have provided a summary and key messages. It's all about women getting consistent information. How they are advised shouldn't depend on where they live or who they go to see. Although we do have to individualize, there are some basic messages that we want to be consistent.
One aim of the British Menopause Society is to support education at the primary care level, but we would love there to be a menopause specialist service within each region. Some women may have complex medical histories that could mean side effects from treatments, in which case there needs to be someone that the primary care can refer to. Whether it's actually referring the patient, whether it's email advice, a phone call or whatever it is, support needs to be provided at a specialist level.
What we want to do is work throughout the country, looking at how we can support people to get the appropriate education. We have training courses to get to that specialist level, so that there can be specialist services within each region. To do that, we also need to work with commissioning groups. This is part of the whole idea about raising awareness of menopause, to try and encourage funding to provide these services.
Where can readers find more information?
There is the British Menopause Society website, which is aimed at healthcare professionals, but it also links to Women's Health Concern, which is the patient charity arm of the British Menopause Society.
In addition, there is Menopause Matters and we publish a magazine as well. There's quite a new website called managemymenopause.co.uk, which gives women more tailored information. This allows people to put in their history, their circumstances and then print off more of an individualized advice sheet.
For women who have premature menopause, there's a support group called the Daisy Network, which is specifically for younger women. They all link together and complement each other. They all provide something a bit different and we don't mind which ones women use. They might want to look at them all and they're all really useful resources.
About Dr Heather Currie
 Dr Heather Currie, Associate Specialist Gynaecologist at Dumfries and Galloway Royal Infirmary, Scotland, specialising in Menopause, Pre Menstrual syndrome and Sub-fertility. Co- Editor of Post Reproductive Health, the Journal of the British Menopause Society (BMS), Chair of the BMS and Managing Director of Menopause Matters Ltd which runs the award winning website www.menopausematters.co.uk, and publishes the award winning Menopause Matters magazine. Author of the award winning book, Menopause, answers at your fingertips and of many original papers and review articles in scientific journals.
Dr Heather Currie, Associate Specialist Gynaecologist at Dumfries and Galloway Royal Infirmary, Scotland, specialising in Menopause, Pre Menstrual syndrome and Sub-fertility. Co- Editor of Post Reproductive Health, the Journal of the British Menopause Society (BMS), Chair of the BMS and Managing Director of Menopause Matters Ltd which runs the award winning website www.menopausematters.co.uk, and publishes the award winning Menopause Matters magazine. Author of the award winning book, Menopause, answers at your fingertips and of many original papers and review articles in scientific journals.
 New commentary urges patient-centered AI regulation in healthcare systems
New commentary urges patient-centered AI regulation in healthcare systems