Asthma care continues to develop, particularly in how treatment and long-term management are approached.
This article outlines current treatment and management recommendations for patients aged 12 and over, along with tailored pathways for managing asthma in children under 5. It also offers practical, guideline-based strategies to help clinicians manage asthma more effectively across different age groups.
Treatment for patients ages 12 and over
Patients with asthma have historically been told to carry their blue inhaler at all times because this will help to keep them safe in the event of an asthma attack. This precautionary step is no longer stipulated in the new guidelines.
Rather, the guidelines state that people aged 12 and above with a new diagnosis of asthma should be offered Anti-Inflammatory Relief (AIR) therapy, with a formoterol-containing inhaled steroid inhaler used by patients on an as-required basis. It is important to note, however, that this process is recommended for someone who is not experiencing symptoms at the time of presentation.
This step should be skipped if a patient is unwell or exacerbating, with the patient instead offered low-dose Maintenance and Reliever Therapy (MART). This asthma treatment plan leverages a single combination inhaler, which is used rather than separate preventer and reliever inhalers.
Patients that continue to be symptomatic after a period of time on a low-dose MART regime should be offered a moderate-dose MART regime. Adherence, inhaler technique, and new triggers should be assessed if this new regime does not relieve symptoms.
If a person is still symptomatic at this point, it is important to understand the symptoms’ cause. For example, this may be uncontrolled eosinophilic airway inflammation, or the inflammation may be controlled and the patient is experiencing bronchospasm.
A FeNO test will be used to measure the patient's FeNO level, with a referral to an asthma care specialist required if this level is raised.
If the FeNO level is not raised, it is recommended that the patient be offered either a Long-Acting Muscarinic Antagonist (LAMA) or a Leukotriene Receptor Antagonist (LTRA) on top of a moderate-dose MART regimen for a period of 8-12 weeks.
Symptoms should be reviewed at the end of the 8-12 weeks:
- If asthma is well controlled, continue with the current regimen.
- If there’s some improvement but symptoms are still present, either continue the current treatment or add the other option (LTRA or LAMA), depending on which one the patient isn’t already taking.
- If there’s no improvement, stop the current add-on (LTRA or LAMA) and switch to the alternative.
The patient should be referred to a specialist if the asthma remains uncontrolled after following these steps.
Nothing needs to change for patients with an existing asthma diagnosis who are currently receiving treatment recommended in the previous guidelines, so long as the asthma is controlled and a relatively small amount of salbutamol is being used.
Should the patient only be using salbutamol with no other inhalers, however, it may be prudent to move them over to an AIR regime.
Patients on a low-dose inhaled steroid who are not using a MART regimen and later become symptomatic should be moved to a low-dose MART regimen. Patients on a moderate-dose steroid should then go to a moderate-dose MART regimen.
If the patient continues to experience symptoms after these steps, it is essential that they are referred to a specialist. Patients who are symptomatic despite using a high-dose steroid should also be referred.
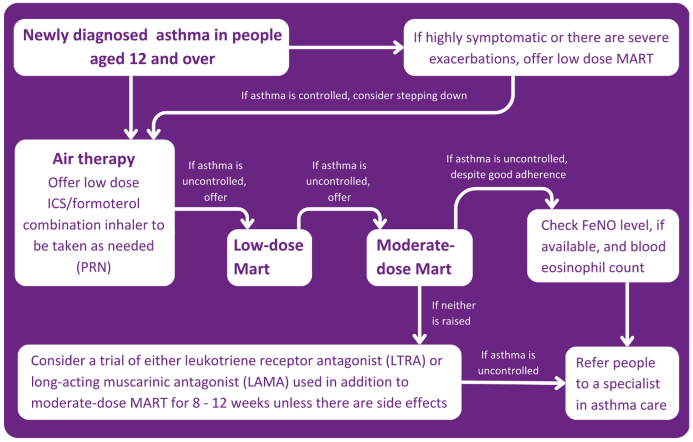
Image Credit: Bedfont® Scientific Ltd
The guidelines also highlight the need to address the possible reasons why the asthma is uncontrolled before adjusting or changing any medication, for instance:
- Alternative diagnosis or comorbidities
- Psychosocial factors
- Seasonal factors
- Environmental factors
- Suboptimal adherence
- Inhaler technique
- Active or passive smoking
Treatment for children (5-11 years)
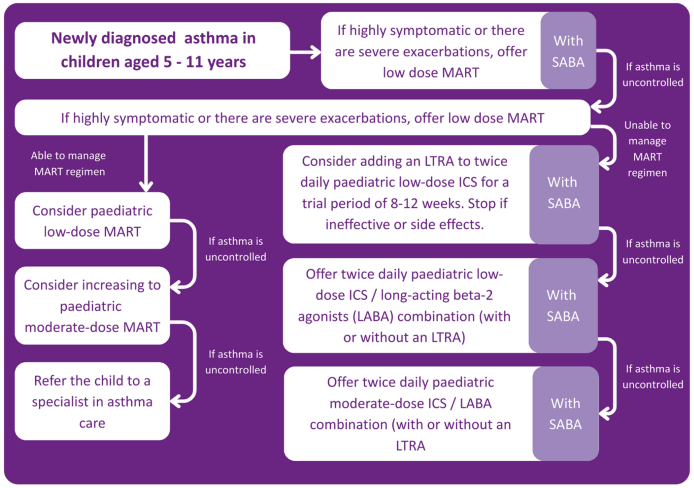
Image Credit: Bedfont® Scientific Ltd
No inhalers are currently licensed for MART in children, though the guidelines do currently advise considering MART in treatment.
MART can be prescribed off-label even though the licensing is not currently available. Under these circumstances, it should be documented that the medication is being used off-label in accordance with the current guidelines by NICE/BTS/SIGN (2024).
Treatment for children under 5
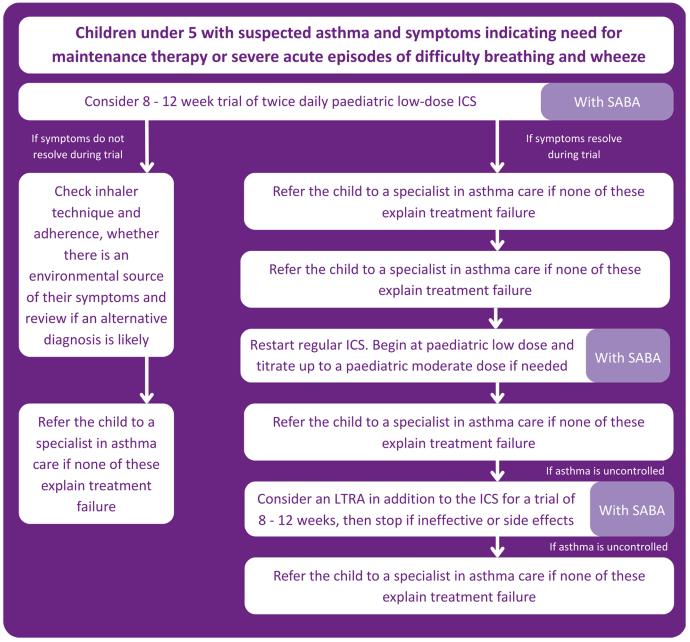
Image Credit: Bedfont® Scientific Ltd
The importance of QOF
The Quality and Outcomes Framework (QOF) had previously required spirometry and one other test to be conducted, but this requirement has now changed in line with the current guidance.
A number of patients newly diagnosed with asthma are now required to have had one of the following tests:
- Eosinophil count
- FeNO
- Spirometry
- Peak flow with Bronchodilator Response (BDR)
- Bronchial responsiveness (in adults)
- Skin prick test or blood IgE (in children)
This should have been done between 3 months before or 3 months after diagnosis, with the diagnosis correctly coded in order to qualify for QOF points.
Monitoring asthma
Asthma control should be monitored at every asthma review by asking these questions:
- Has there been any absence from school or work due to asthma?
- How much is a reliever inhaler being used? This should be asked along with a check of the prescription record.
- How many courses of oral corticosteroids have been used?
- Have there been any emergency visits or hospital admissions due to asthma?
The guidelines advise the use of an asthma control test at reviews, specifying that peak flow should not be used to assess asthma control unless there is a person-specific reason to do this.
The guidelines also state that FeNO testing should be considered in reviews for adults, both prior to and following changes in asthma medication.
Poor asthma control
If a patient has poor asthma control, it is recommended to check their FeNO level, as this may be a major indicator of their poor adherence to treatment or the need for an increased dose of Inhaled Corticosteroids (ICS).
A Short-Acting Beta2 Agonist (SABA) should no longer be prescribed without an ICS, and if any change to asthma medication is made, you should review the response within 8-12 weeks.
Changing medication
Guidance is now available to help select the most appropriate inhaler for a patient, with considerations including:
- The patient’s ability to use the inhaler correctly
- The patient's preference around inhalers
- The lowest environmental impact among appropriate devices
- The presence of or need for a dose counter
The guidelines also stipulate that a spacer should be prescribed with a metered dose inhaler, especially in children.
If control deteriorates or the inhaler changes, it is important to check inhaler technique as part of an asthma review. If the patient cannot use the device correctly, a more suitable alternative should be selected.
Risk care
HCPs are advised to identify asthma patients who face a greater risk of poor outcomes, with risk factors including:
- Non-adherence to medication
- Overuse of SABA inhalers (for example, more than two a year)
- Requiring two or more courses of corticosteroids a year
- Two or more hospital admissions or emergency visits for asthma a year
It is also important to note that the guidelines recommend evaluating patients who are more at risk, and HCPs should not forget about the other patients.
Summary
The most recent guidelines from NICE, BTS, and SIGN introduced major changes around the diagnosis and management of asthma.
It may initially be challenging to adapt to these updates, but proper education and resources are key to helping healthcare professionals effectively integrate these changes.
This unified approach will enhance asthma care in the long term, improving outcomes for thousands of patients.
About Bedfont® Scientific Ltd
Bedfont® Scientific has specialised in the design and manufacture of exhaled breath and gas monitoring instruments since 1976.
For medical gas monitoring, their Medi-Gas Check medical pipeline testing range verifies not only the quantity but also quality of gas administered to patients.
Bedfont's breath analysers include carbon monoxide (CO) monitors such as the Smokerlyzer®, used for smoking cessation, and the ToxCO®, used by emergency services, to diagnose CO poisoning.
The NObreath® FeNO monitor provides accurate analysis of airway inflammation for the control of asthma, and the Gastrolyzer® range aids in the detection of gastrointestinal disorders and food intolerances. Quick and non-invasive, breath analysis is the new blood test.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.Net which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.