The Fractional Exhaled Nitric Oxide (FeNO) test has long been part of clinical guidelines and was a key element in the previous asthma care recommendations from the National Institute for Health and Care Excellence (NICE).
However, until recently, the British Thoracic Society (BTS) and the Scottish Intercollegiate Guidelines Network (SIGN) only endorsed FeNO for confirming an asthma diagnosis. Now, in a unified update, all three organizations – NICE, BTS, and SIGN – have recommended FeNO as a first-line diagnostic tool for asthma.
Nitric Oxide (NO) is a naturally occurring gas that we exhale as part of normal respiratory function. In individuals with eosinophilic airway inflammation, a common feature of asthma, NO levels are elevated, leading to a higher FeNO reading.
This makes the FeNO test a valuable indicator in assessing airway inflammation and guiding asthma diagnosis.
Occupational asthma
There are no new updates in the guidelines regarding occupational asthma; instead, they refer clinicians to the British Thoracic Society (BTS) clinical statement on the topic.
However, the guidelines do emphasize the importance of considering occupational triggers, particularly in cases of adult-onset asthma or when a patient’s asthma is poorly controlled.
Clinicians are advised to ask patients the following questions to help assess potential work-related symptoms:
- Are your symptoms the same, better, or worse on days away from work?
- Are your symptoms the same, better, or worse during holidays or extended breaks from work?
If symptoms appear to worsen at work and occupational asthma is suspected, referral to a specialist is recommended.
Asthma diagnosis in children (Aged 5-16)
Once a clear history and physical examination have taken place and asthma is suspected, it is possible to carry out tests. This approach is the same as with adults.
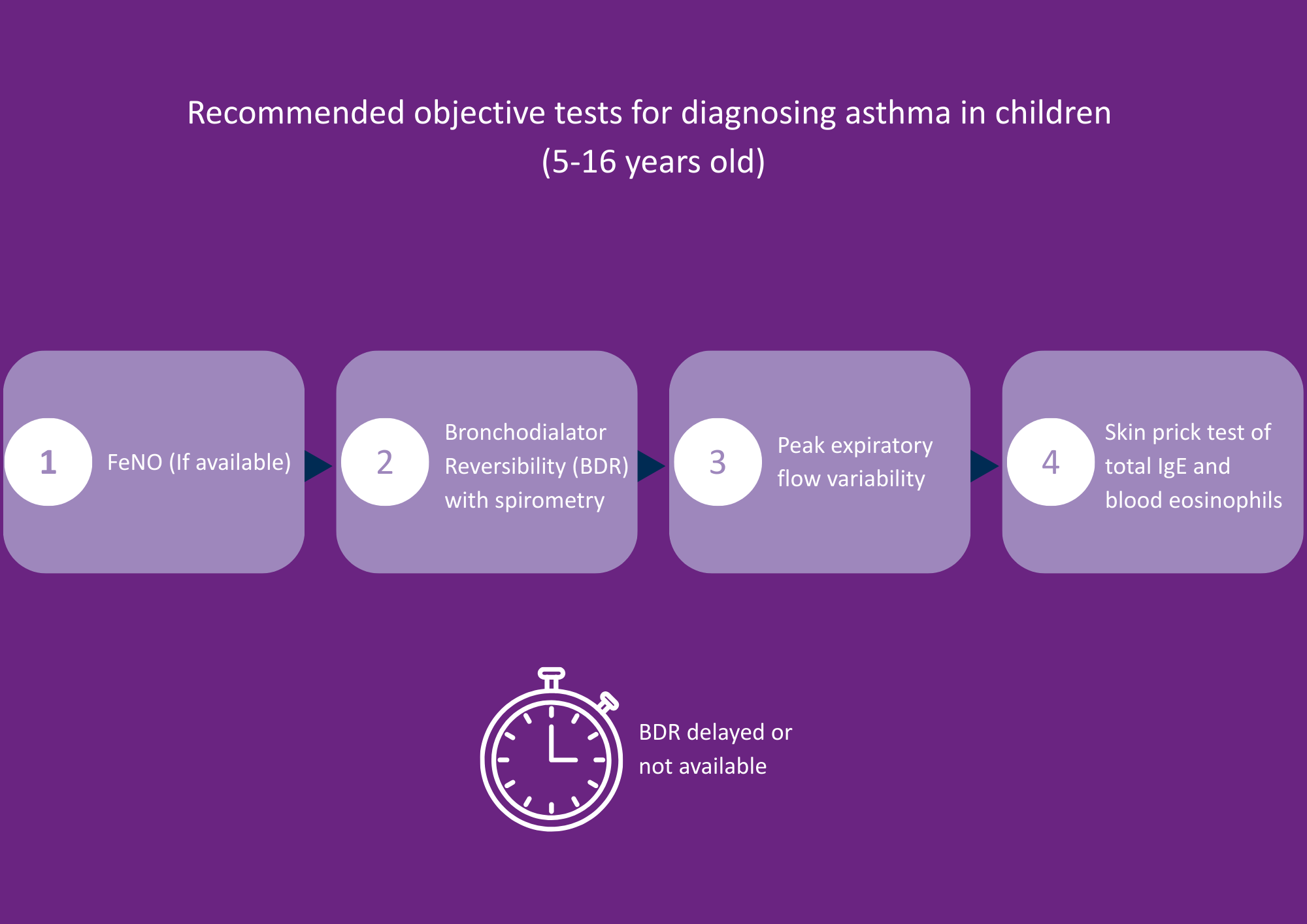
Image Credit: Bedfont® Scientific Ltd
A FeNO test is the first and only recommended test for children, meaning that a FeNO device should be available in primary care settings.
- If the FeNO result does not support an asthma diagnosis, the next step is bronchodilator reversibility (BDR) testing with spirometry. However, younger children may find this test difficult to perform reliably.
- If spirometry isn’t feasible, the guidelines suggest using a peak flow diary to monitor variability in lung function over time.
- If peak flow results are inconclusive, a skin prick test is the next recommended step. That said, access to skin prick testing is limited in many areas, which may make this option unavailable.
- Blood eosinophil testing is considered a last resort due to its invasive nature.
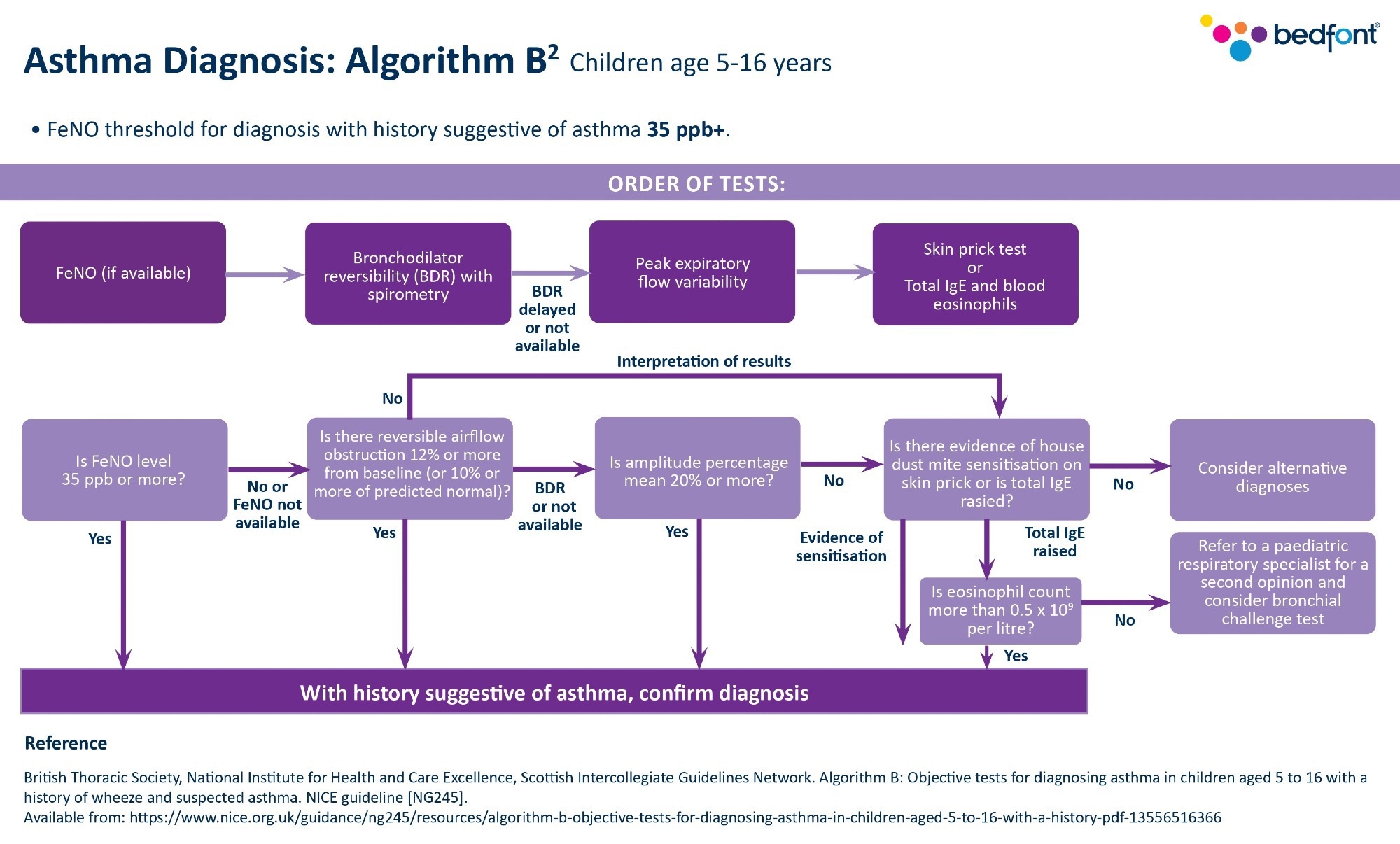
Image Credit: Bedfont® Scientific Ltd
How to incorporate FeNO testing
In some Primary Care Networks (PCNs), nursing teams offer short, same-day appointments specifically for FeNO testing. In these settings, the entire nursing team is trained to perform the test and accurately code the results.
However, this model isn’t always feasible in every practice. In such cases, the alternative approach is to ensure all clinicians are trained to carry out FeNO testing themselves.
This means that patients can receive instant results, start treatment immediately in the same appointment, and be referred to the asthma specialist for a follow-up.
Children under 5 years old
Healthcare professionals (HCPs) had previously advised not to diagnose asthma in children under 5 years old, instead waiting until the child was 5 years old before making a diagnosis.
The new guidelines recognize the challenges associated with diagnosing this age group, because young children do not possess the breath control required for testing. Recommendations in the new NICE/BTS/SIGN guidelines are as follows:
- Use clinical judgement to treat and review regularly if asthma is suspected.
- Attempt to test for asthma once the patient reaches 5 years old. It is unclear whether treatment should stop prior to the test, however.
- Continue treatment with regular reviews if the test is unsuccessful.
- Re-attempt testing every 6-12 months.
- Refer the patient to a specialist if they are not responding to treatment, as this could be a key indicator that the child does not have asthma.
The guideline also recommends that any preschool child admitted to the hospital or who has had two or more emergency care visits because of respiratory issues in 12 months be referred to a specialist.
Next steps
With a clearer understanding of FeNO testing and its applications, it is now important to focus on how these new guidelines reshape asthma treatment and long-term management.
About Bedfont® Scientific Ltd
Bedfont® Scientific has specialised in the design and manufacture of exhaled breath and gas monitoring instruments since 1976.
For medical gas monitoring, their Medi-Gas Check medical pipeline testing range verifies not only the quantity but also quality of gas administered to patients.
Bedfont's breath analysers include carbon monoxide (CO) monitors such as the Smokerlyzer®, used for smoking cessation, and the ToxCO®, used by emergency services, to diagnose CO poisoning.
The NObreath® FeNO monitor provides accurate analysis of airway inflammation for the control of asthma, and the Gastrolyzer® range aids in the detection of gastrointestinal disorders and food intolerances. Quick and non-invasive, breath analysis is the new blood test.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.Net which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.