Since the onset of the coronavirus disease 2019 (COVID-19) pandemic, several variants of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have emerged that have consistently replaced the previous dominant variant. Understanding the changes associated with infection by new SARS-CoV-2 variants is considered important from public health, clinical, and basic science perspectives.
 *Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
Background
SARS-CoV-2 variants of concern (VOCs) are associated with increased transmissibility, case severity, and/or antigenic differences. The three VOCs that most significantly impacted the COVID-19 pandemic include the SARS-CoV-2 Alpha (B.1.1.7), Delta (B.1.617.2), and Omicron (B.1.1.529) variants.
Before the emergence of the Omicron variant, the Delta sublineage AY.4.2 replaced the other Delta lineages and was assumed to become the dominant strain in the United Kingdom in early 2022. However, its spread was arrested by the subsequent emergence of the Omicron variant.
The severity of a disease caused by a pathogen upon entry into a new host species from a zoonotic reservoir is generally quite far from its evolutionary optima. For SARS-CoV-2, individuals of a younger age are associated with lower virulence, while severe diseases have been reported to a greater degree in older age groups and those with comorbidities. Therefore, factors determining transmission and immune evasion are most likely considered to determine the direction of evolution rather than the evolution of virulence.
A new study published on the preprint server medRxiv* aimed to determine how the severity of successively dominant SARS-CoV-2 variants has changed since the beginning of the pandemic.
About the study
The current study involved the generation of genome sequences using the ARTIC Network protocol for different variants at different time frames. For the Alpha analysis, all sequenced genomes with full metadata between November 1, 2020, and January 30, 2021, were included, whereas the Alpha/Delta analysis included all sequenced samples with full metadata between April 1, 2021, and June 30, 2021.
For the Delta/AY.4.2 analysis, all sequenced samples with full metadata between July 1, 2021, and October 31, 2021, were studied, whereas the non-AY.4.2 Delta/Omicron analysis included all sequenced samples with full metadata between December 1, 2021, and December 31, 2021. All sequences were obtained from individuals younger than 18 years of age, with hospital-acquired COVID-19 patients excluded from the study.
The researchers also collected other linked data such as hospital admission information, date of admission, date of discharge from the hospital, sex, age at diagnosis, number of vaccine doses, reinfection, and number of comorbidities. The severity of infection for the different variants was also assessed.
Study findings
Confirmed Alpha cases were associated with more severity as compared to the previous dominant non-VOC lineage (B.1.177), with 37.2% of analyzed Alpha infections having severe outcomes or being hospitalized.
An increase in case severity was observed with the Delta infections as compared to Alpha, with 6.7% of cases having severe outcomes or being hospitalized from Delta infections. Furthermore, infections caused by the AY.4.2 lineage were found to have similar severity to the other Delta sublineage infections. The infections caused by Omicron were found to be less severe as compared to the previous variants.
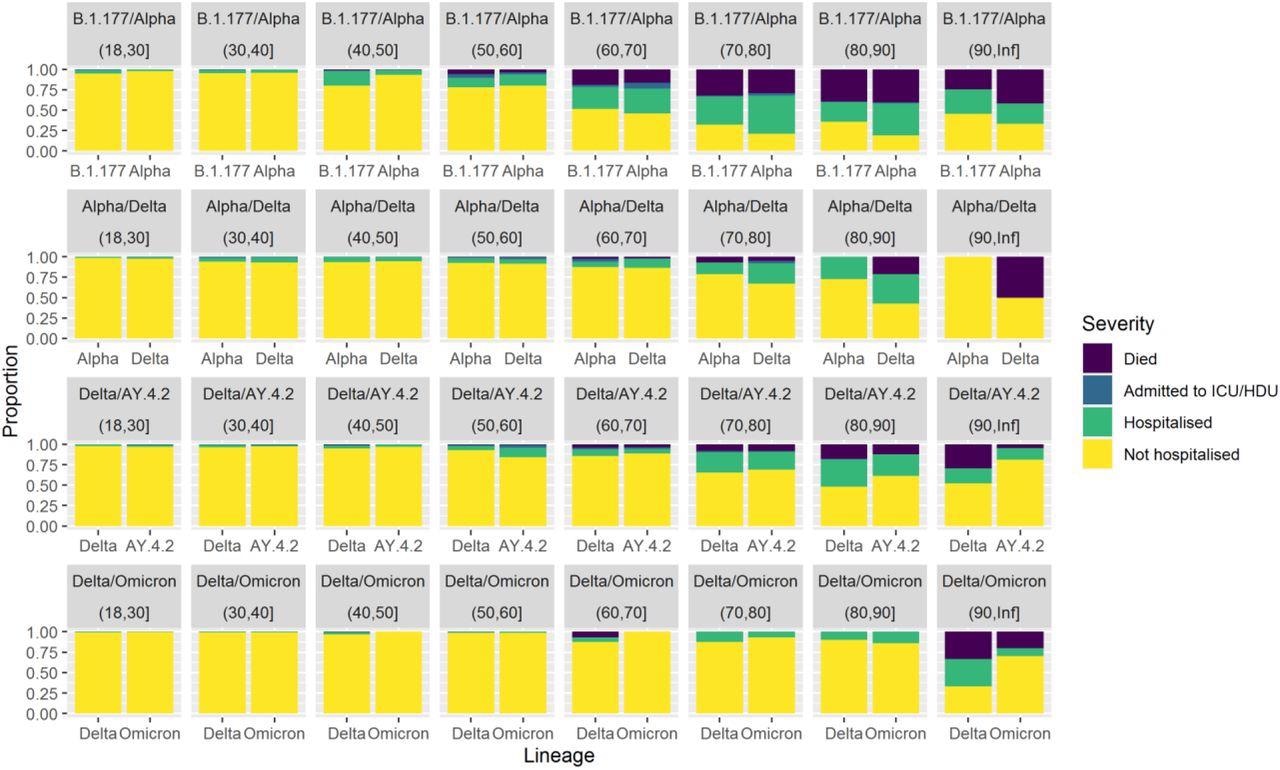
Comparison of case severity by age between pairs of co-circulating SARS-CoV-2 lineages. Clinical severity was measured on a four-level ordinal scale based on observed outcomes within 28 days of a positive test: no hospitalisation, hospitalisation, admission to ICE/HDU, death. The first row compares B.1.177 and Alpha between 1st November 2020 and 30th January 2021. The second row compares Alpha and Delta between 1st April 2021 and 30th June 2021. The third row compares Delta lineages against AY.4.2 between 1st July 2021 and 30th September 2021. The fourth row compares non-AY.4.2 Delta and Omicron between 1st December 2021 and 31st December 2021.
Conclusions
The current study demonstrates that the successive variants of SARS-CoV-2 were associated with inconsistent differences in disease severity. Therefore, the historical trends in severity cannot be used in the prediction of the severity of future variants. However, genome sequencing can help estimate the likelihood of immune evasion and the method of cell entry for new variants.
Limitations
Samples with only a sequenced genome are included in the study; therefore, the samples mostly include cases with lower Ct. A second limitation of the current study was the small sample size.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
 Emerging SARS-CoV-2 variant BA.3.2 shows no signs of greater danger
Emerging SARS-CoV-2 variant BA.3.2 shows no signs of greater danger