Introduction
How potassium supports nerve, muscle, and heart function
How processed foods contribute to potassium deficiency
The health risks of inadequate potassium intake
Dietary strategies to improve potassium intake
Key takeaways
References
Further reading
Modern diets dominated by processed, sodium-rich foods have contributed to widespread inadequate potassium intake, a nutritional pattern linked to higher risks of hypertension, stroke, cardiovascular disease, and mortality.
 Image Credit: Katyam19 / Shutterstock.com
Image Credit: Katyam19 / Shutterstock.com
Introduction
Despite potassium's essential role in a wide range of physiological functions, approximately 86% of the global population consumes less than the WHO target of more than 3.5 g/day; this is usually due to inadequate dietary intake rather than clinical potassium deficiency.1 This widespread nutritional imbalance has significant implications for cardiovascular, metabolic, renal, and skeletal health, particularly in populations consuming sodium-rich processed foods.
How potassium supports nerve, muscle, and heart function
Potassium is the primary intracellular cation in the human body. It is primarily concentrated in muscle tissue and bones, as well as the kidneys, gastrointestinal tract, heart, and central nervous system. This essential element maintains fluid homeostasis, acid-base balance, and normal cell function, in addition to its well-characterized physiological role in electrochemical signaling.
In excitable cells, a tightly regulated potassium concentration gradient exists between the intracellular and extracellular compartments to support nerve impulse propagation and coordinated cardiac and skeletal muscle contraction. Small perturbations in this gradient can result in clinically significant arrhythmias, impaired muscle function, and altered neural excitability.5
Within the cardiovascular system, increased plasma potassium concentrations lead to endothelium-dependent vasodilation, which is partly mediated by stimulation of the adenosine triphosphatase (ATPase) sodium-potassium pump and opening of potassium channels.3 In the kidneys, potassium promotes sodium excretion and reduces intravascular volume to counteract the vascular effects of excess sodium, including arterial stiffening and impaired nitric oxide synthesis.6
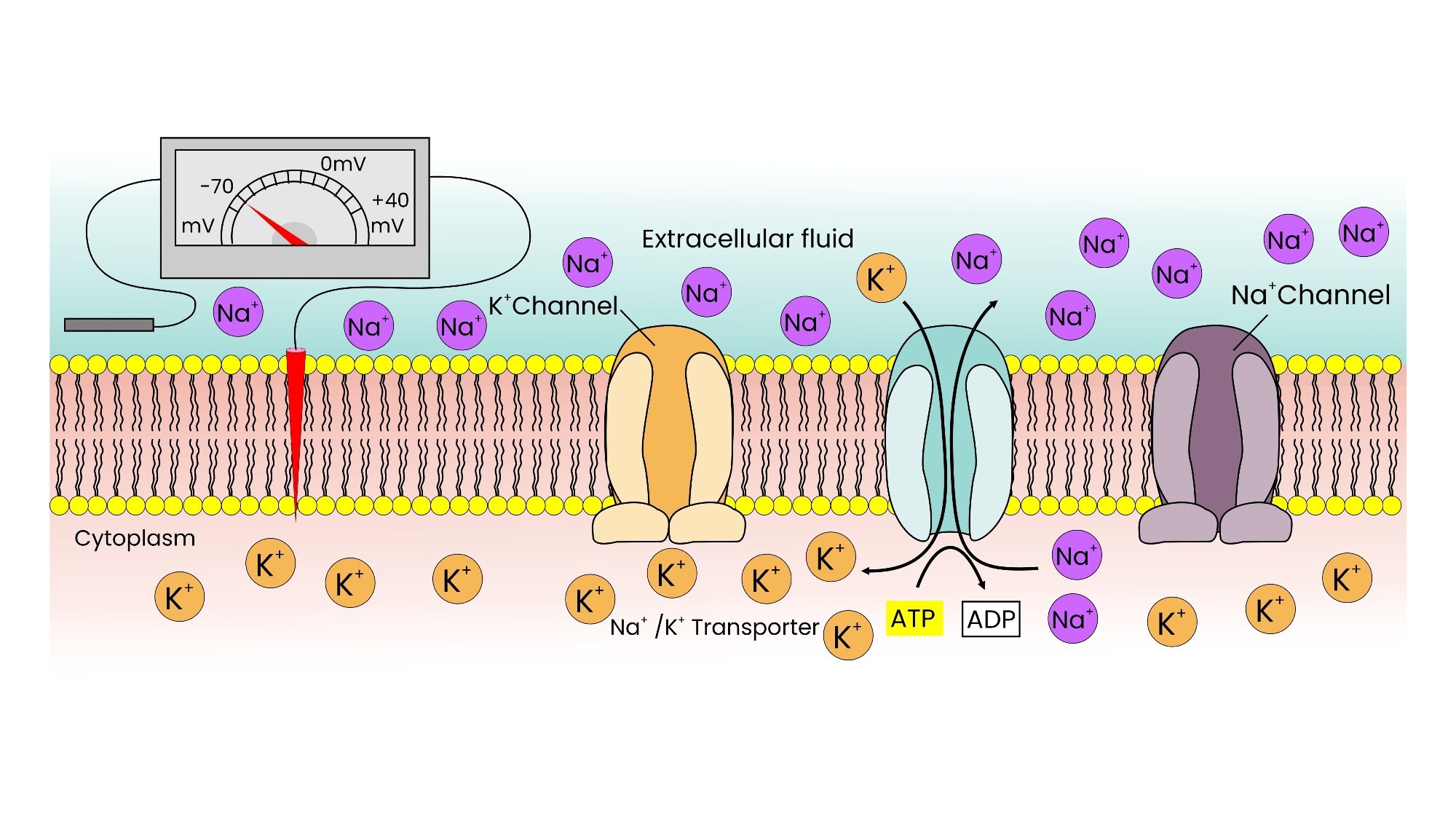 Image Credit: GigVenture / Shutterstock.com
Image Credit: GigVenture / Shutterstock.com
How processed foods contribute to potassium deficiency
The global shift towards increased consumption of highly processed foods directly contributes to the widespread prevalence of low potassium intake, as these products are often high in sodium with negligible potassium content.5 Socioeconomic factors compound these trends, with higher-potassium dietary patterns linked to the consumption of fresh fruits, vegetables, and legumes, many of which are foods that are not readily available to lower-income populations.1,5
A systematic review of data from 52 countries and over 1.6 million participants estimated a global mean potassium intake of 2.25 g/day, which is significantly less than the World Health Organization (WHO) recommendation of more than 3.5 g/day.1 In the United States, only 3% of Americans obtain sufficient potassium through their diet, with the average American consuming just over half the recommended amount.3
In pre-agricultural populations, dietary potassium intake often exceeded 200 mmol/day, while sodium intake was comparatively low, resulting in a potassium-to-sodium molar ratio of at least 3, comparable to the current ratio of 0.4 in Western countries.3
The National Health and Nutrition Examination Survey (NHANES) data indicate that American men consume an average of 4.3 g of sodium and 3.4 g of potassium every day. In contrast, women consume 2.9 g of sodium and 2.4 g of potassium.6 Globally, the lowest mean potassium intake has been reported in East Asia at 1.9 g/day, whereas the highest-intake region of Eastern Europe reports 3.5 g/day.1
The health risks of inadequate potassium intake
Experimental data suggest that a potassium-rich diet may increase endothelial nitric oxide production and suppress reactive oxygen species, potentially conferring cardiovascular protection beyond blood pressure regulation.2 Notably, the benefits of increased potassium intake on blood pressure appear to be greatest in individuals with high sodium consumption, making the sodium-to-potassium ratio a key measure of diet-related cardiovascular risk.3,4,6
Whereas increased potassium intake lowers systolic blood pressure, inadequate potassium intake increases the risk of stroke.4 Specifically, a 24% reduced risk of incident stroke has been observed in individuals with higher potassium intake, with each additional 10 mmol increase in daily intake associated with 40% lower stroke-associated mortality risk.3,4
Longitudinal data from the NHANES Linked Mortality File, which followed 12,267 adults for approximately 15 years, found that higher sodium-to-potassium ratios were independently associated with 46% higher cardiovascular disease mortality and 115% higher ischemic heart disease mortality.6 Significant correlations between potassium intake and metabolic health have also been reported, with observational evidence suggesting lower type 2 diabetes risk at daily intakes between 3,000 and 5,000 mg, although the relationship appears J-shaped rather than simply linear.2
Potassium from organic salts may attenuate age-related bone loss by modulating renal acid excretion and reducing urinary calcium loss, with evidence also suggesting potential benefits for bone health and kidney stone risk.3 Furthermore, NHANES data suggest that low potassium intake was associated with an 18% higher mortality risk.5 However, people with advanced chronic kidney disease or impaired renal potassium handling require individualized guidance, because hyperkalemia can cause malignant arrhythmias and sudden cardiac death, even though the direct relationship between dietary and serum potassium remains unclear.5
Dietary strategies to improve potassium intake
Vegetables rich in potassium include beet greens, sweet potatoes, tomato puree, Swiss chard, spinach, and acorn squash. Bananas are also potent sources of potassium, with over 400 mg per serving, as are other fruits like peaches, prunes, and avocado.7
Legumes such as white beans, soybeans, and lima beans, as well as dairy products such as nonfat plain yogurt, are high in potassium. Wild Atlantic salmon has a high potassium content, averaging 534 mg per three-ounce serving.7
For populations where whole-food potassium intake is constrained by affordability, potassium-enriched salt substitutes are a practical intervention. The Salt Substitute and Stroke Study demonstrated reductions in cardiovascular events and mortality after regular salt was replaced with a reduced-sodium, potassium-enriched salt substitute, so the observed benefit likely reflects both lower sodium and higher potassium exposure.1,2 This strategy is not appropriate without medical guidance for people with impaired renal potassium handling or those using medications that raise potassium.5,7 Notably, greater reliance on plant-based potassium was associated with better survival outcomes as compared to those who primarily obtained potassium from animal-based products, irrespective of kidney function status, possibly because plant sources also provide fiber and other cardiometabolic nutrients.5
 Image Credit: Elena Eryomenko / Shutterstock.com
Image Credit: Elena Eryomenko / Shutterstock.com
Key takeaways
Potassium plays a crucial role in cardiovascular regulation, renal function, skeletal metabolism, and glucose homeostasis, underscoring the systemic importance of adequate potassium intake.4,5 Despite its importance, modern diets that rely heavily on processed foods have led to the inversion of the dietary potassium-to-sodium ratio, which has broad clinical relevance.1,4
For populations where socioeconomic barriers limit access to fresh vegetables and fruits, targeted strategies, including salt substitution, should be leveraged as public health tools. These strategies should prioritize potassium-rich whole foods and caution against supplements or potassium-containing salt substitutes in people at risk of hyperkalemia.5,7 In the future, long-term randomized controlled trials are needed to fully characterize dose-response relationships and clarify the role of potassium in outcomes beyond cardiovascular disease.2
References
- Reddin, C., Ferguson, J., Murphy, R., et al. (2023). Global mean potassium intake: a systematic review and Bayesian meta-analysis. European Journal of Nutrition 62(5); 2027-2037. DOI: 10.1007/s00394-023-03128-6. https://link.springer.com/article/10.1007/s00394-023-03128-6.
- D'Elia, L. (2024). Potassium intake and human health. Nutrients, 16(6), 833. DOI: 10.3390/nu16060833. https://www.mdpi.com/2072-6643/16/6/833.
- Weaver C. M. (2013). Potassium and health. Advances in Nutrition, 4(3), 368S–77S. DOI: 10.3945/an.112.003533. https://www.sciencedirect.com/science/article/pii/S2161831322011279?via%3Dihub.
- Aburto, N. J., Hanson, S., Gutierrez, H., et al. (2013). Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ 346. DOI: 10.1136/bmj.f1378. https://www.bmj.com/content/346/bmj.f1378.
- Narasaki, Y., You, A. S., Malik, S., et al. (2022). Dietary potassium intake, kidney function, and survival in a nationally representative cohort. The American Journal of Clinical Nutrition 116(4); 1123-1134. DOI: 10.1093/ajcn/nqac215. https://www.sciencedirect.com/science/article/pii/S0002916523036304
- Yang, Q., Liu, T., Kuklina, E. V., et al. (2011). Sodium and potassium intake and mortality among US adults: prospective data from the Third National Health and Nutrition Survey. Archives of Internal Medicine 171(13); 1183-1191.
DOI: 10.1001/archinternmed.2011.257. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1106080
- National Heart, Lung, and Blood Institute. (2020, September 1). DASH eating plan: Getting More Potassium Fact Sheet.
Accessed from: https://www.nhlbi.nih.gov/resources/getting-more-potassium-fact-sheet
Further Reading
Last Updated: Jun 9, 2026
 Why potatoes and grains can’t replace each other in a healthy diet
Why potatoes and grains can’t replace each other in a healthy diet