In the U.S., Blacks, Hispanics, and other indigenous populations have been historically marginalized. Compared to White individuals, these racial and ethnic (RE) groups have also been at two to three times greater risk of COVID-19-related hospitalization and nearly two times greater COVID-19 mortality risk. Even for the general population, incarceration increases the COVID-19 mortality rate by three-fold and case rates by 5.5-fold. Hence, it is not surprising that incarceration has emerged as a critical risk factor for COVID-19 morbidity and mortality in these RE groups.
Although the impact of COVID-19 among incarcerated RE groups is highly disproportionate, data supporting RE inequities in COVID-19 metrics among incarcerated populations is limited. The data from most carceral systems and even U.S. Departments of Corrections (DOCs) is unregulated; therefore, it rarely helps assess metrics stratified by RE or other demographics. Thus, greater data transparency from all carceral systems is needed to understand populations at disproportionate risk of COVID-19 mortality.
About the study
In the present retrospective population-based study, researchers from Harvard Medical School, Brigham and Women’s Hospital, and Harvard T. H. Chan School of Public Health obtained data from the U.S. DOCs by filing Freedom of Information Act (FOIA) requests to estimate the rate of COVID-19 cases and deaths among incarcerated RE individuals in the U.S. state prisons. They collected RE data for person-level COVID-19 cases, death, and custody population between March 1 and October 1, 2020.
The team submitted FOIA requests on October 1, 2020, and curated data on June 1, 2021. Further, they supplemented the study data with publicly available data, e.g., third-party organizations, such as the Texas Justice Initiative. From states that provided sufficient data for the study of COVID-19 mortality estimates, the researchers subsequently requested the age distribution of the custody population by RE to enable age standardization. They collected race and ethnicity data per DOC's classification to categorize the study population into Hispanic and non-Hispanic groups.
The researchers calculated crude RE-specific cumulative COVID-19 death rates per 1,000 persons state-wise. For aggregated COVID-19-related mortality rate calculations, they used the race-specific prison population on March 1, 2020, as the denominator. Further, the team used Whites as the reference group for calculations of rate ratios (RR). Across RE categories, they used a one-way analysis of variance to compare the mean age of a person dying due to COVID-19 and the same statistical method with a Bonferroni correction for pairwise comparisons.
The researchers calculated age-standardized COVID-19 mortality rates by aggregating deaths and custody populations into age-race-state strata. However, due to a lack of age-based case data, they could not determine COVID-19 case rates stratified by age. Since age-stratified data varied by state, they assigned a midpoint of the age range to each age category for modeling comparisons. In some cases, they also used publicly available data to determine a midpoint of the age range.
Finally, the team used a negative binomial model to estimate death counts. The model used random intercepts for states and modeled age as a second-order polynomial. Furthermore, it added an indicator variable for race/ethnicity and an offset for the natural log of the population.
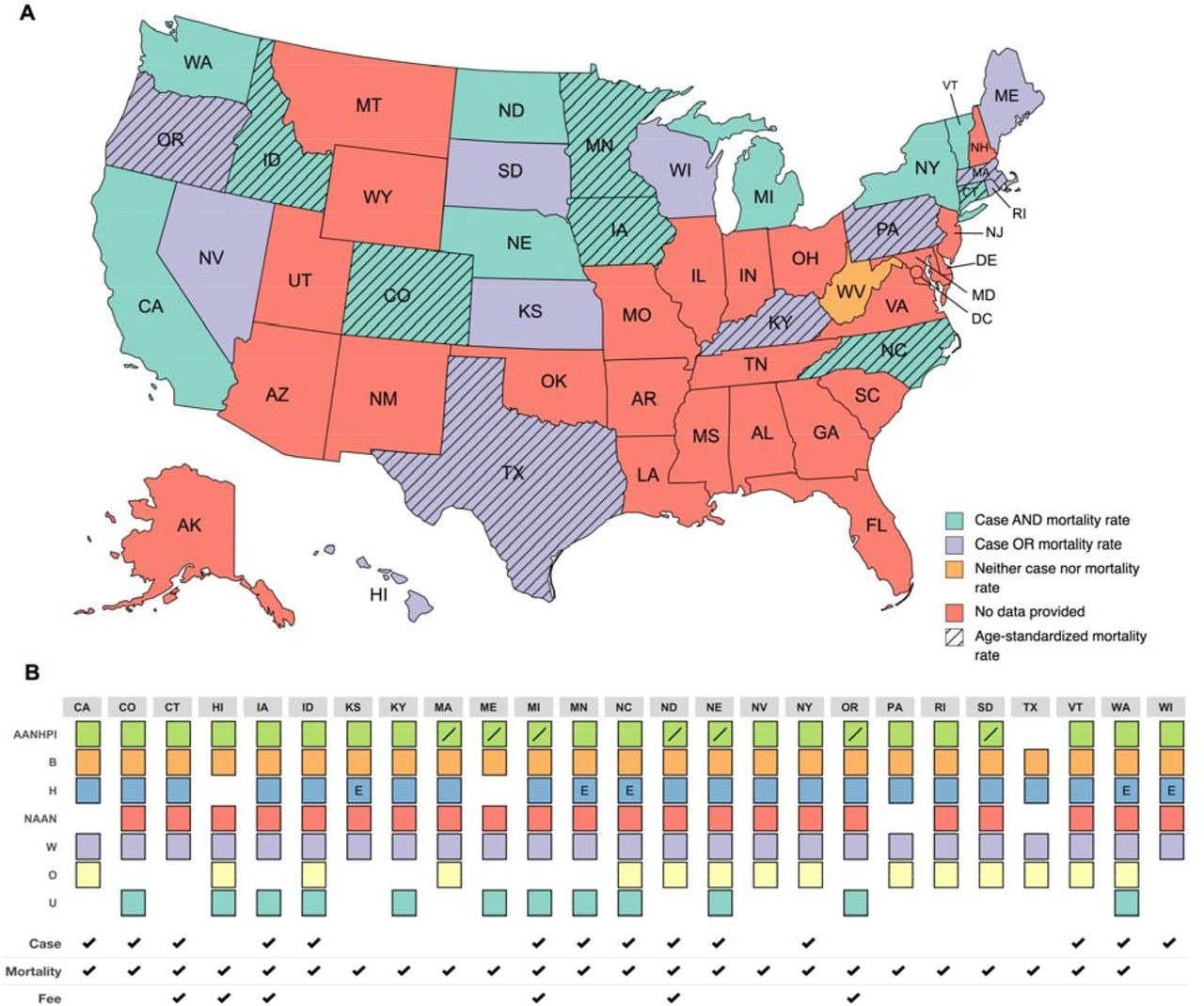
Data, Race, and Ethnicity Reporting from State DOCs Abbreviations: Asian American, Native Hawaiian, and Pacific Islander (AANHPI), Black (B), Hispanic (H), Native American and Alaskan Native (NAAN), White (W), Other (O), and Unknown (U) (Top) States sending at least partial data are displayed. Figure displays whether each state provided data sufficient to calculate case and mortality rates, case or mortality rates, neither case nor mortality rates, age-standardized mortality rates, or no data at all. States that sent 3/01/2021 custody population, 10/01/2021 case and mortality data by race/ethnicity (all RE groups for case data; White, Black, Hispanic, at minimum for mortality data) were considered having sent all data for case and mortality rate calculations. States that additionally sent mortality data by age are indicated as having sent all data necessary for calculating age-standardized mortality rates. (Bottom) Displays the data sets and racial/ethnic categories reported by each state. States that requested fees are also indicated. States that sent SARS-CoV-2 case (“Case”) and/or mortality data (“Mortality”) by race/ethnicity are marked. Forward slash denotes states that reported Asian American, Native Hawaiian, and Pacific Islander in disaggregated racial categories. “E” denotes states reporting “Hispanic” as an ethnicity rather than a race category.
Study findings
The authors filed FOIA requests with all 50 state DOCs; however, only 19 states provided crude COVID-19 mortality rates, while only 11 states provided adequate data for age-standardized COVID-19 mortality rates calculations. Additionally, each state's DOCs had varying racial and ethnic classifications.
Of all the COVID-19-related deaths in the U.S. prisons through October 2020, the study could capture only 23.35% of deaths (272/1165). The authors observed varied crude mortality rates across all the U.S. state prisons, ranging from 17 to 142 per 100,000 people in Colorado and Texas, respectively. Compared to the White population, Hispanics had a significantly greater aggregate COVID-19 mortality rate.
The average age for COVID-19 mortality was 63 years. However, the average age was lower among Black than White adults (60 years vs. 63 years). Compared to Whites, age-standardized COVID-19 mortality rates were highest among Black individuals, with RR=1.93. The mortality rates were also higher among Hispanic and other RE groups, with RRs of 1.81 and 2.60, respectively.
Conclusions
According to the authors, this is the first study to provide a granular understanding of RE inequities in COVID-19 metrics across U.S. state prisons. To summarize, among incarcerated individuals, the rate of COVID-19-related mortality in Black and Hispanics were 93% and 81% higher than in White individuals. Further, there were striking RE inequities in overall COVID-19 mortality and younger age at death for the Black population.
The study highlighted the need for mandatory data transparency and standardized reporting of COVID-19 data stratified based on demography. This data could help inform policies to safeguard the marginalized RE groups in prisons and cease high COVID-19 transmissions and deaths over time.
 This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Journal references:
- Preliminary scientific report.
Examining COVID-19 Mortality Rates by Race and Ethnicity Among Incarcerated People in U.S. State Prisons, Mimi Yen Li, Shelby Grebbin, Ankita Patil, Tori Cowger, Dennis Kunichoff, Justin M. Feldman, Monik Jimenez, medRxiv pre-print 2022, DOI: https://doi.org/10.1101/2022.06.24.22276470, https://www.medrxiv.org/content/10.1101/2022.06.24.22276470v1
- Peer reviewed and published scientific report.
Li, Mimi Yen, Shelby Grebbin, Ankita Patil, Tori L. Cowger, Dennis Kunichoff, Justin Feldman, and Monik C. Jiménez. 2022. “Examining COVID-19 Mortality Rates by Race and Ethnicity among Incarcerated People in 11 U.S. State Prisons (March–October 2021).” SSM - Population Health 20 (December): 101299. https://doi.org/10.1016/j.ssmph.2022.101299. https://www.sciencedirect.com/science/article/pii/S2352827322002786.
 Ten-million-person study links semaglutide to lower COVID-19 mortality
Ten-million-person study links semaglutide to lower COVID-19 mortality