Introduction
What is the placenta?
Developmental origins of health and disease (DOHaD)
Placental structure and function predicting future health
Placental function and epigenetic programming
Maternal environment, placental health, and offspring outcomes
Clinical implications of placenta-based predictions
Research gaps and future directions
References
Further reading
The placenta plays a central role in fetal development by regulating nutrient transfer, hormonal signaling, and immune interactions, thereby shaping lifelong health outcomes. Evidence from developmental programming research indicates that placental structure and function, as well as environmental exposures during pregnancy, can predict cardiometabolic disease risk later in life.
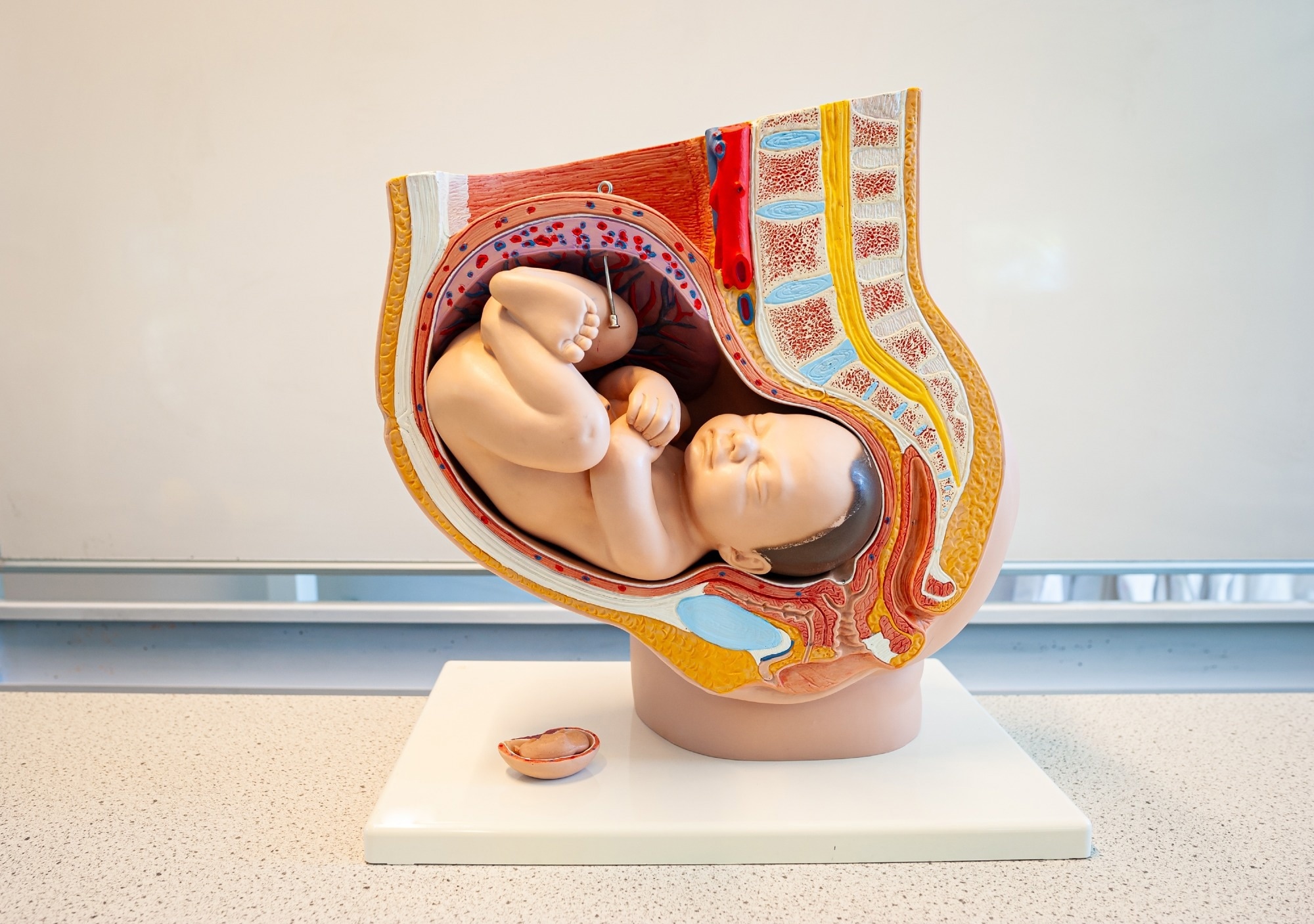 Image Credit: Menno van der Haven / Shutterstock.com
Image Credit: Menno van der Haven / Shutterstock.com
Introduction
Disruptions in placental development or nutrient exchange can have lasting effects that increase an infant’s risk of developing chronic diseases later in life. As a key regulator of fetal growth and development, placental function may also predict lifelong cardiometabolic risk, thus emphasizing the importance of optimizing maternal health during pregnancy.2 The placenta acts as a dynamic interface that senses maternal environmental signals, including nutrition, metabolic status, endocrine signals, stress, and environmental exposures, and translates them into developmental cues that influence fetal physiology and long-term disease susceptibility.7
What is the placenta?
Although transient, the placenta is a complex organ that serves as the biological interface between the mother and the fetus. Specifically, the placenta mediates the transfer of oxygen and nutrients, removes fetal waste products, and produces hormones, including human chorionic gonadotropin (HCG), placental growth hormone, progesterone, and estrogen, that are essential for the onset and maintenance of pregnancy. The organ develops from the embryonic trophectoderm and contains branching villous structures composed of trophoblast layers surrounding fetal capillaries, enabling efficient exchange between the maternal and fetal circulations.3
The placenta also supports immune function through tightly regulated interactions between maternal immune cells and fetal trophoblasts. When this balance is disrupted, immune mismatch may contribute to implantation failure, pregnancy loss, preeclampsia (PE), or preterm birth.3,4
Under optimal placental function, maternal nutrient supply is sufficient to support fetal growth requirements. However, if the placenta is under stress due to poor maternal nutrition, metabolic disease, inflammation, hypoxia, or vascular dysfunction, it may alter nutrient transport, hormone production, or immune signaling. These adaptations also have the potential to interfere with the development of fetal organs such as the heart, pancreas, kidneys, and brain.3 Importantly, many placental responses represent adaptive mechanisms that adjust fetal growth to match maternal resource availability rather than purely pathological changes.7
Developmental origins of health and disease (DOHaD)
The Developmental Origins of Health and Disease (DOHaD) framework proposes that environmental exposures during early development determine lifelong health trajectories. Specifically, the body responds to environmental cues by altering gene expression, which, if misregulated, increases the risk of metabolic disorders. Within this framework, the placenta functions as a sensor and regulator of maternal environmental signals that influence fetal metabolic programming and developmental pathways.1,7
This concept emerged from the pioneering work of David Barker, who proposed the “Barker hypothesis” in 1995. The Barker hypothesis associates fetal undernutrition in middle to late gestation with disproportionate fetal growth, which can increase the risks of cardiovascular disease, hypertension, stroke, and type 2 diabetes in adulthood. Birth weight is often used as a proxy for the intrauterine environment, reflecting the placenta's ability to supply nutrients and oxygen during fetal development.2
Evolutionary perspectives also suggest that the placenta mediates a balance between maternal and fetal interests, a concept known as “maternal constraint,” in which nutrient transfer to the fetus may be regulated to preserve maternal health and future reproductive success.2
Developmental origins of health and disease (DOHaD)
Placental structure and function predicting future health
Placental morphology and function have been widely studied for their impact on long-term health outcomes. Variations in placental shape may also provide insights into potential differences in vascular development and nutrient delivery that influence fetal growth trajectories.
Although a larger placenta size generally supports greater fetal growth, placental efficiency more closely reflects adequacy. A disproportionately large placenta relative to birth weight suggests compensatory adaptation to a suboptimal maternal environment that may increase cardiometabolic risk later in life.2 Studies have demonstrated that an increased placental-to-birth-weight ratio is associated with higher blood pressure and cardiovascular disease risk later in life.7
Gross features such as placental thickness, shape, and umbilical cord insertion provide important indicators of the placental adequacy and efficiency during fetal development. Microscopically, villous architecture and vascular branching determine oxygen and nutrient exchange. Impaired vascularization or placental growth restriction can reduce fetal blood supply and alter kidney development, which can increase the risk of hypertension in adulthood.2,5 These structural changes are often linked to abnormalities in placental vascular remodeling, particularly incomplete transformation of maternal spiral arteries, which can limit uteroplacental blood flow.5
Experimental studies also suggest the existence of a “placenta–heart axis,” in which impaired placental perfusion and altered hemodynamics during development can influence fetal cardiovascular development and long-term cardiometabolic health.7
 Image Credit: Sinhyu Photographer / Shutterstock.com
Image Credit: Sinhyu Photographer / Shutterstock.com
Placental function and epigenetic programming
Alterations in placental structure or function can determine health trajectories across the lifespan through epigenetic mechanisms, which are heritable modifications in gene expression that occur without affecting the underlying deoxyribonucleic acid (DNA) sequence. Epigenetic changes, such as DNA methylation of growth-related genes, including insulin-like growth factor 1 (IGF-1), may alter pathways involved in metabolism, vascular function, and endocrine regulation.
Placental dysfunction linked to hypoxia, oxidative stress, maternal obesity, diabetes, or hypertensive disorders can further induce epigenetic changes in fetal organs that may predispose offspring to cardiometabolic diseases.3,4 For example, the presence of hypertensive disorders of pregnancy (HDP), including PE, has been implicated in epigenome-wide DNA methylation, particularly affecting genes related to developmental and neurological pathways. Large population studies have identified multiple CpG sites associated with HDP exposure in cord blood, although the observed methylation differences are typically modest, suggesting subtle but potentially biologically meaningful epigenetic effects.6
Maternal environment, placental health, and offspring outcomes
Maternal metabolic and inflammatory conditions like gestational diabetes mellitus (GDM), obesity, and HDP, including PE, can alter placental nutrient transport, vascular development, oxygen delivery, and endocrine signaling.1 GDM, for example, can arise due to the activity of placental hormones that increase maternal insulin resistance and pancreatic beta-cell demand. Changes in placental transporter activity, including systems responsible for amino acid, glucose, and fatty acid transfer, may alter fetal nutrient supply and contribute to abnormal growth patterns.7
Comparatively, impaired uteroplacental perfusion, oxidative stress, and antiangiogenic signaling characterize PE. PE is associated with a greater likelihood of fetal growth restriction (FGR), oligohydramnios, and preterm birth, which increase the risk of respiratory distress syndrome, intraventricular hemorrhage, sepsis, bronchopulmonary dysplasia, and neurodevelopmental disabilities in the infant.3,4
Chronic low-grade inflammation is a characteristic feature of obesity, which is accompanied by other metabolic disturbances, such as increased oxidative stress, insulin resistance, and elevated cortisol levels. Maternal obesity predisposes the mother to GDM, placental dysfunction, and adverse pregnancy outcomes, including large- and small-for-gestational-age babies. Although placental 11β-hydroxysteroid dehydrogenase-2 (11β-HSD2) reduces excess cortisol exposure to the fetus, severe stress or other pathologies may disrupt this protective mechanism, exacerbating metabolic dysfunction.3,4
 Image Credit: karegg / Shutterstock.com
Image Credit: karegg / Shutterstock.com
Clinical implications of placenta-based predictions
Placental biology may offer significant diagnostic potential to predict both maternal health conditions and long-term fetal health outcomes. For example, first-trimester markers like pregnancy-associated plasma protein-A (PAPP-A) have been associated with abnormal placental development and adverse pregnancy outcomes such as fetal growth restriction and preeclampsia. In contrast, low levels of PAPP-A have been associated with short stature and later maternal diabetes.3
Angiogenic factors, specifically a high soluble fms-like tyrosine kinase-1 (sFlt-1) to placental growth factor (PlGF) ratio, significantly improve the prediction, diagnosis, and management of PE and FGR. Altered β-hCG alevels nd emerging biomarkers, such as epidermal growth factor-like domain 7 (EGFL7), have also been investigated for their utility in monitoring placental dysfunction throughout gestation.3 These biomarkers reflect underlying disturbances in placental angiogenesis and vascular function.5
These insights reinforce the importance of optimizing maternal nutrition, metabolic health, stress management, and environmental exposures to support placental function. Similarly, placenta-based screening and prevention strategies could enable early identification of placental risk markers, enabling timely and targeted maternal interventions and thereby limiting intergenerational transmission of cardiometabolic risk and the long-term burden of chronic disease.2,3
Research gaps and future directions
Longitudinal studies that monitor maternal-offspring pairs across decades are needed to establish causal links between placental function and adult disease risk. Despite their resource-intensive nature and logistical demands, these studies are essential for clarifying the mechanisms by which early placental adaptations lead to measurable health outcomes later in life.1
At the mechanistic level, further research is needed to delineate the molecular and cellular pathways that regulate placental development, vascularization, nutrient sensing, and endocrine signaling. Although strong epidemiological links exist, the biological mechanisms underlying associations between placental morphology, exchange efficiency, and cardiometabolic and neurodevelopmental risk remain unclear.2,3
Integrative approaches, including systems biology and mathematical modeling of placental exchange dynamics, may enhance prognostic precision. Furthermore, incorporating placental structural and functional parameters into predictive models could enable individualized risk stratification and advance precision medicine.2,3 Advances in imaging technologies and molecular profiling may also enable earlier detection of placental dysfunction during pregnancy.4
References
- Giachini, F. R., Hryciw, D. H., Castro-Parodi, M., & Damiano, A. E. (2024). Editorial: The placenta: The origin of chronic diseases in adults. Frontiers in Endocrinology 15. DOI: 10.3389/fendo.2024.1455965. https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2024.1455965/full
- Lewis, R., Cleal, J., & Hanson, M. (2012). Review: Placenta, evolution, and lifelong health. Placenta 33; S28-S32. DOI: 10.1016/j.placenta.2011.12.003. https://www.sciencedirect.com/science/article/abs/pii/S0143400411005753
- Ortega, M. A., Fraile-Martinez, O., Garcia-Montero, C., et al. (2022). The Pivotal Role of the Placenta in Normal and Pathological Pregnancies: A Focus on Preeclampsia, Fetal Growth Restriction, and Maternal Chronic Venous Disease. Cells 11(3). DOI: 10.3390/cells11030568. https://www.mdpi.com/2073-4409/11/3/568
- Nelson, D. M., & Myatt, L. (2020). The Human Placenta in Health and Disease. Obstetrics and Gynecology Clinics of North America 47(1). DOI: 10.1016/j.ogc.2020.01.001. https://www.sciencedirect.com/science/article/abs/pii/S0889854520300012
- Benagiano, M., Mancuso, S., Brosens, J. J., & Benagiano, G. (2021). Long-Term Consequences of Placental Vascular Pathology on the Maternal and Offspring Cardiovascular Systems. Biomolecules 11(11). DOI: 10.3390/biom11111625. https://www.mdpi.com/2218-273X/11/11/1625
- Kazmi, N., et al. (2019). Hypertensive Disorders of Pregnancy and DNA Methylation in Newborns. Findings from the Pregnancy and Childhood Epigenetics Consortium, Hypertension 74(2); 375-383. DOI: 10.1161/HYPERTENSIONAHA.119.12634. https://www.ahajournals.org/doi/10.1161/HYPERTENSIONAHA.119.12634
- Cleal, J. K., Poore, K. R., & Lewis, R. M. (2022). The placental exposome, placental epigenetic adaptations and lifelong cardio-metabolic health. Molecular Aspects of Medicine 87; 101095. DOI: 10.1016/j.mam.2022.101095. https://www.sciencedirect.com/science/article/pii/S0098299722000401
Further Reading
Last Updated: Mar 8, 2026
 Researchers uncover sex-specific metabolic patterns in ocular tissues
Researchers uncover sex-specific metabolic patterns in ocular tissues