 This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
VL influences SARS-CoV-2 secondary transmission. Higher VL has been attributed, at least in part, to the emergence of Alpha and Delta VOCs.
Furthermore, with segments of the population having received vaccines, understanding VL in breakthrough infections post-vaccination is critical. Studies on the presence of infectious viruses by cell culture isolation are important, as RNA VL is a weak indicator for infectiousness.
About the study
In the current study, up to five days post-onset of symptoms (DPOS), the researchers examined viral load features in the upper respiratory tract (URT) of unvaccinated pre-VOC-infected coronavirus disease 2019 (COVID-19) participants, as well as vaccinated and unvaccinated Delta VOC-infected COVID-19 subjects. In this cohort, 384 samples were included, with 118 samples acquired from patients infected with the pre-VOC SARS-CoV-2 and 248 from patients infected with the Delta VOC.
A total of 121 of the Delta VOC-infected patients had been vaccinated twice prior to their infection, whereas 127 had not been vaccinated. The study also included 18 vaccinated people who had recently been infected with Omicron. Using quantitative real-time PCR (qRT-PCR) and a focus-forming assay, the researchers measured genome copies and infectious viral titers in SARS-CoV-2-positive nasopharyngeal swabs.
The researchers first examined whether RNA genome copies are a good predictor of infectious viral shedding. They then determined whether infectious viral loads in patient samples were related to patient age and gender.
Over the first five symptomatic days, the researchers compared genome copies and infectious viral levels in pre-VOC and Delta VOC samples from unvaccinated patients. They further evaluated genome copies and infectious viral loads in non-vaccinated and vaccinated patients infected with the Delta VOC throughout the first five days after infection to determine whether immunization had an effect on virus shedding.
The researchers also investigated infectious viral shedding in vaccinated patients infected with the novel VOC Omicron strain after it emerged. In nasopharyngeal swab samples obtained from 18 Omicron- and 17 Delta-infected patients, RNA, and infectious viral load levels were also compared.
Study findings
The results showed that unvaccinated Delta-infected individuals had a greater infectious viral load than pre-VOC infected patients and that vaccinated patients had a much lower infectious viral load. There was no difference in infectious viral load between Delta and Omicron breakthrough cases.
RNA genome copies in URT swab samples were only weakly linked with infectious virus shedding. In fact, the researchers discovered more RNA genome copies in the swabs of unvaccinated individuals infected with pre-VOC SARS-CoV-2 strains than the Delta VOC within the first five DPOS. At the same time, Delta VOC had greater infectious viral titers.
During the first five days after symptom onset, the researchers were able to show that infectious viral load, rather than RNA genome copies, is reduced in vaccinated Delta VOC patients. Furthermore, approximately 50% of transmissions for pre-VOC SARS-CoV-2 strains occur during this time frame, thereby indicating that a reduction in viral load could significantly contribute to a lower secondary attack rate.
According to the data, the higher transmissibility of the SARS-CoV-2 Omicron variant is not associated with the shedding of a larger number of infectious viral particles in vaccinated patients with equivalent RNA viral load and infectious virus shedding.
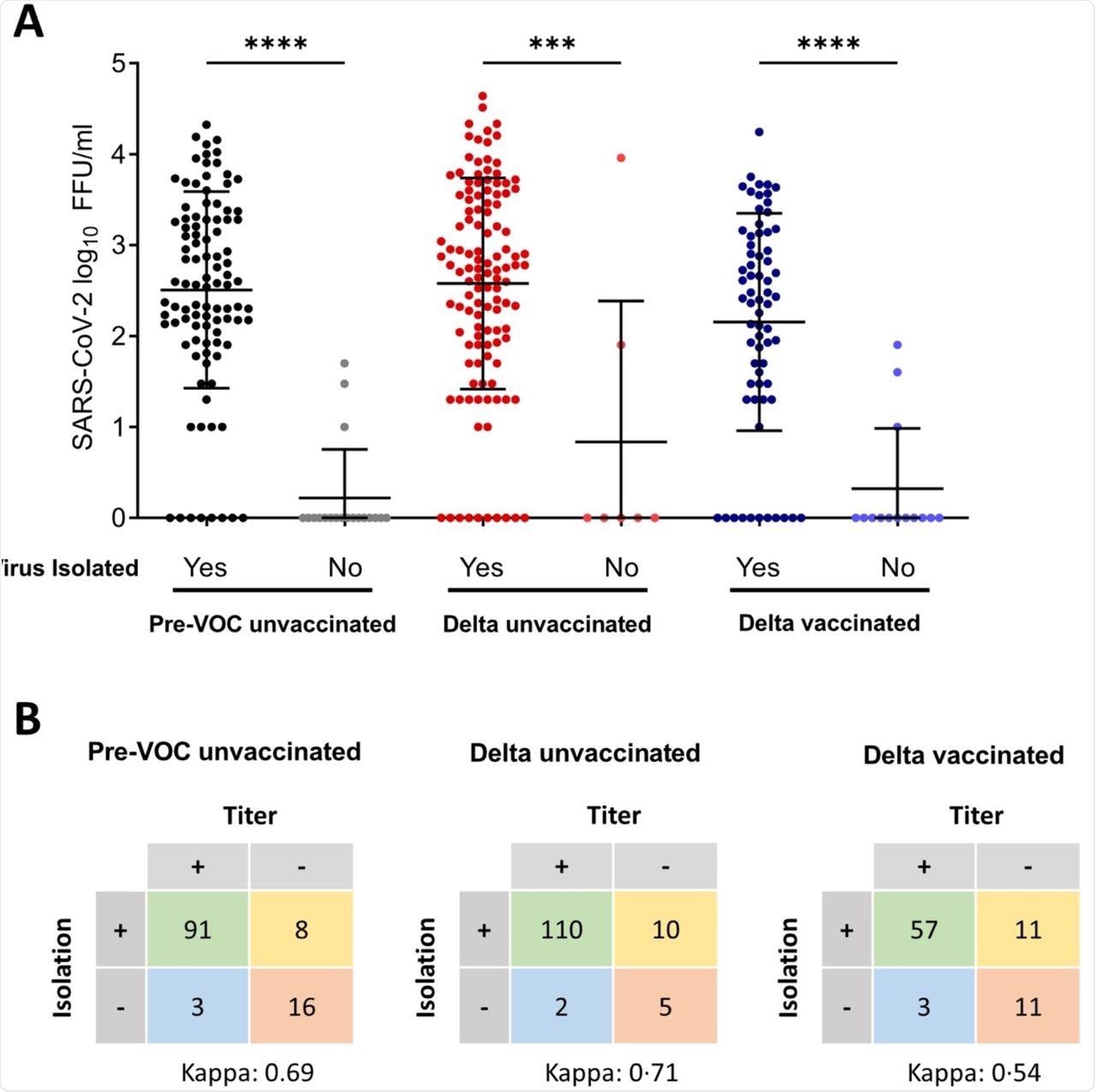
Quantitative infectious viral loads versus overall virus isolation success.
Limitations
Only samples with cycle threshold (Ct) values less than 27 were included and were obtained within the first five DPOS, but not later. As patients with low viral loads were not included, absolute counts on RNA copies are skewed toward larger viral loads.
Furthermore, the researchers were concentrated on infectious virus shedding. To this end, it was demonstrated that SARS-CoV-2 culture is unlikely to be successful from samples with higher Ct values and that the vast majority of secondary transmission occurs before five DPOS. However, this needs to be formally assessed in Omicron cases.
The researchers also did not have access to samples from Omicron-infected unvaccinated people due to the recent emergence of this strain. Finally, the researchers indicated that almost all of the patients in this study were vaccinated with messenger ribonucleic acid (mRNA) vaccines, which produce high neutralizing antibody titers but low mucosal antibodies. As a result, the findings do not apply to other vaccines, especially those used largely in low- and middle-income countries.
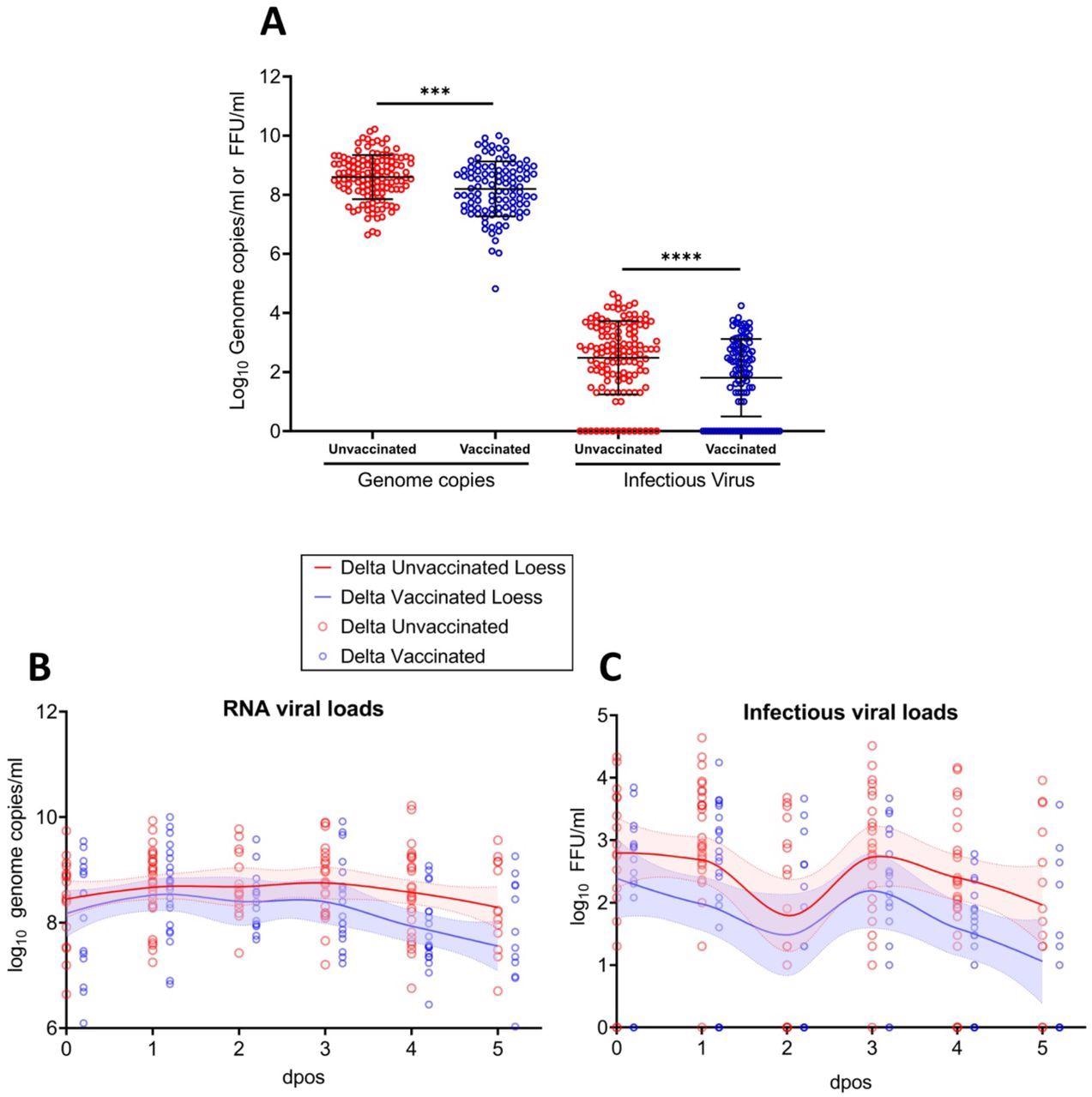
RNA viral load and infectious viral titers for unvaccinated vs. vaccinated individuals infected Delta (A) Genome copies (left panel) and infectious virus (right panel) for vaccinated and unvaccinated Delta infected patients. Error bars indicate mean±SD. The t-test was used to determined differences of means. ***p=0·0005; ****p<0·0001. Genome copies (B) and infectious viral loads (C) measured for vaccinated and unvaccinated Delta infected patients at different dpos. The solid lines represent the fitted curve calculated using (locally estimated scatterplot smoothing) LOESS method.
Conclusions
Taken together, the study results show that the Delta VOC has stronger infectivity but much lower infectivity and faster virus clearance in vaccinated individuals. Furthermore, the findings demonstrated that the Omicron and Delta VOCs have identical infectious viral loads. In addition to overall virus isolation performance, measuring viral loads can also provide superior insights into viral shedding dynamics in acute SARS-CoV-2 infection.
“We observed higher RNA genome copies in pre-VOC SARS-CoV-2 compared to Delta, but significantly higher IVTs in Delta infected individuals.”
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Journal references:
- Preliminary scientific report.
Puhach, O., Adea, K., Hulo, N., et al. (2022). Infectious viral load in unvaccinated and vaccinated patients infected with SARS-CoV-2 WT, Delta, and Omicron. medRxiv. doi:10.1101/2022.01.10.22269010. https://www.medrxiv.org/content/10.1101/2022.01.10.22269010v1.
- Peer reviewed and published scientific report.
Puhach, Olha, Kenneth Adea, Nicolas Hulo, Pascale Sattonnet, Camille Genecand, Anne Iten, Frédérique Jacquérioz Bausch, et al. 2022. “Infectious Viral Load in Unvaccinated and Vaccinated Individuals Infected with Ancestral, Delta or Omicron SARS-CoV-2.” Nature Medicine, April, 1–1. https://doi.org/10.1038/s41591-022-01816-0. https://www.nature.com/articles/s41591-022-01816-0.
 Nearly 70 weeks after infection, long COVID patients show no detectable inflammation in blood tests
Nearly 70 weeks after infection, long COVID patients show no detectable inflammation in blood tests