Vaccines have played a substantial role in mitigating severe COVID-19 and related mortality since their approval for use; however, the efficacy of these vaccines has been found to wane over time. This reduction in protection, along with the emergence of immune-escaping variants of SARS-CoV-2 like the Omicron variant, has raised concerns on how to effectively control the current pandemic.

Study: The value of vaccine booster doses to mitigate the global impact of the Omicron SARS-CoV-2 variant. Image Credit: Oleksandra Klestova / Shutterstock.com
 *Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
Study findings
In the current study, the researchers fitted an immunological model to population-level data on vaccine effectiveness and described the association between neutralizing antibody titers (NAT) and protection against mild and severe COVID-19 over time. To this end, they showed that NAT for Omicron decreased by 3.9-fold as compared to the SARS-CoV-2 Delta variant.
The researchers also re-parameterized the model to add data on NAT and vaccine efficacy after one vaccine dose from clinical trials. Data on the immunogenicity of booster vaccine doses administered between six and eight months after receiving dose two was also included in this model.
Using this model, the researchers predicted that 90 days after receiving a Pfizer-BioNTech booster vaccine, efficacy against severe COVID-19 or hospitalization declines to 95.9% against the Delta variant and 78.8% against the Omicron variant.
The team applied a multiplicative scaling factor to capture the decline in efficacy against the Omicron variant for all vaccines used in the study. As compared to wild type (WT) strain of SARS-CoV-2, NAT reductions for previous variants were 8.8 and 1.6-fold, respectively, while previous studies have shown a six- and 40-fold NAT reduction for WT and Omicron strains of SARS-CoV-2, respectively.
The researchers integrated this immunological model within a SARS-CoV-2 transmission model and demonstrated that the size of the Omicron-led wave is dependent on the extent of previous exposure to SARS-CoV-2 infection across the population. Thus, in countries that have already experienced a large Delta wave, the Omicron wave was relatively small.
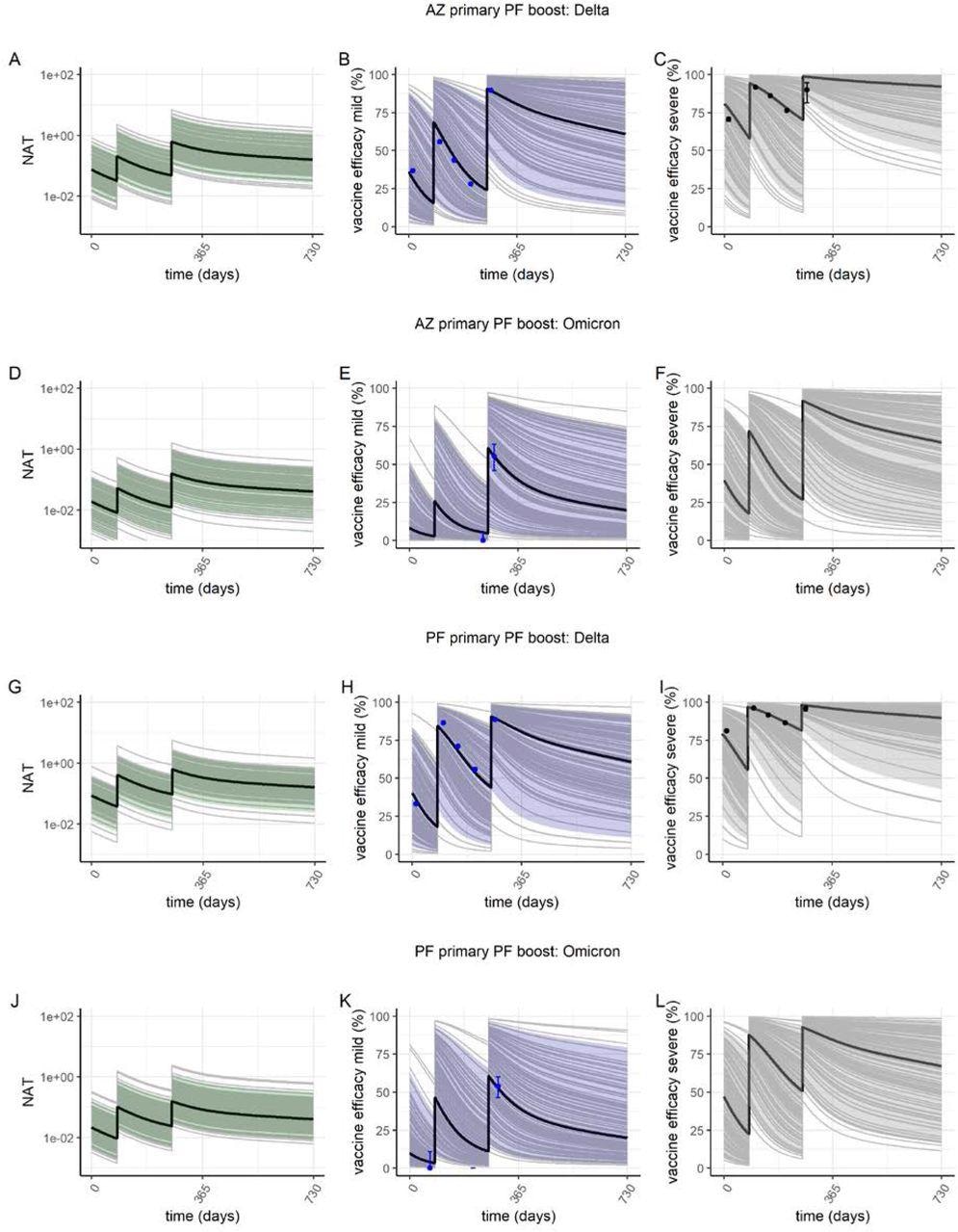
Predicted vaccine efficacy over time. Plots show neutralizing antibody titre (NAT) (green), vaccine efficacy against mild disease (purple) and severe disease (grey) for the AZ-PF regimen (panels A-F) and PF-PF regimen (panels F–L). The solid black line shows the posterior median estimate, colour bands the 95% range of individual responses and grey lines show 100 individual draws from the variation estimated between individuals in (13) illustrating the impact of variability in immune responses across the population. In panels B, E, H and K, the blue points are estimates of vaccine efficacy against mild disease (i.e. PCR+ tested infections which include asymptomatic infections detected through regular screening in schools and some workplaces) with the Delta and Omicron variants in England from (24, 25). In panels C and I, the black points represent vaccine efficacy against hospitalization with the Delta variant from the same source. Panels A–C and G–I show NAT and vaccine efficacy against the Delta variant; panels D–F and J–L show NAT and vaccine efficacy against the Omicron variant.
Global epidemic trajectories based on vaccine access
To study the different epidemic trajectories based on vaccine access, the authors stratified the present epidemiological state of countries into three categories.
In the first setting, countries have experienced significant previous waves of infection, had a high level of infection-induced immunity, and have excellent access to vaccines, with most of the adult population having received two vaccine doses. This category included countries in North America, Central/South America, the Middle East, and most of Europe. In this category, the administration of a booster dose six months after receiving the second vaccine dose to those aged above 60 years substantially reduced hospitalizations and deaths by 32% and 34%, respectively, between January 2021 and the end of 2022 as compared to not providing booster doses and not implementing any NPIs.
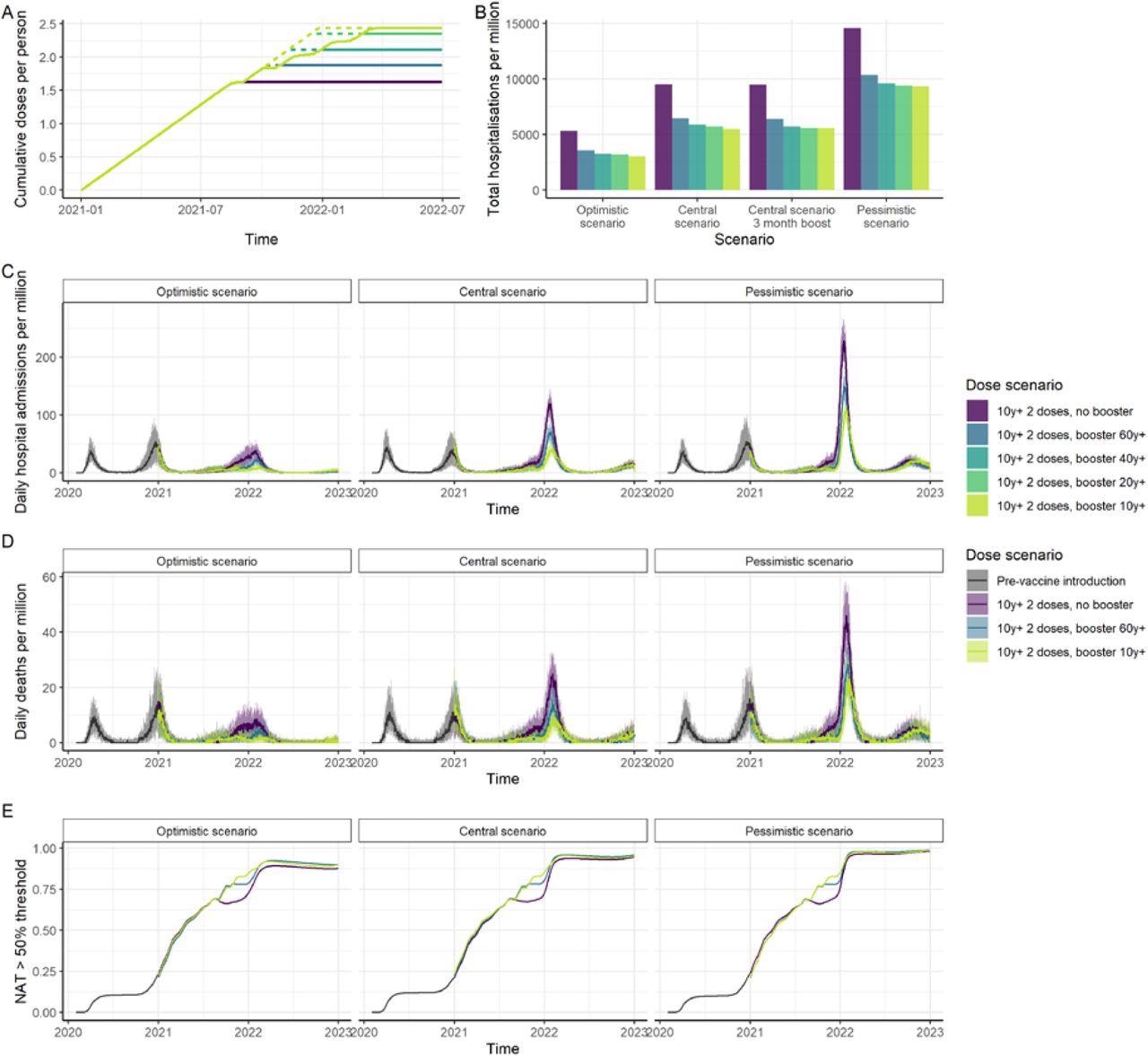
Impact of vaccination in a high-income country setting with substantial prior transmission and high vaccine access. (A) Cumulative vaccine doses delivered per person over time. Solid lines represent a 6-month period between dose 2 and the booster dose; dashed lines represent a 3-month period. Vaccine impact is shown for five dose scenarios: no booster doses, booster doses to those aged 60+, booster doses to those aged 40+, booster doses to those aged 20+ and booster doses to those aged 10+. Impact is shown for three epidemiological scenarios: central, with our central estimate of the VFR (3.9), Omicron Rt=3.5 (the same as Delta) and the risk of hospitalization reduced by 50% for Omicron compared to Delta; optimistic with our lower estimate of VFR (2.9), Omicron Rt=3.25 and risk of hospitalization reduced by 70%; and pessimistic with our upper estimate of the VFR (5.5), Rt=3.75 and risk of hospitalization reduced by 40%. All scenarios assume 90% vaccine uptake in each group and the risk of death further reduced by 58% from the risk of hospitalization. (B) Total hospitalizations per million post-vaccine introduction at the beginning of 2021 through to end-2022, for the central, best-case and worst-case scenarios, and assuming a 6-month period between dose 2 and the booster, except where specified. (C) Daily hospital admissions; and (D) Daily deaths per million population for the best-case, central, and worst-case scenarios. (E) Proportion of the population with NAT higher than the titre relative to convalescent required to provide 50% protection from infection, for the central VFR estimate.
The second category included countries with substantial prior transmission and infection-induced immunity, but with limited access to vaccines. In this scenario, prioritizing the limited booster vaccine supply in the elderly higher-risk group had a greater public health impact in reducing hospitalizations and deaths by 8% and 9%, respectively, as compared to using limited booster doses to boost younger age groups in an attempt to reduce viral transmission.
The third category included “zero-COVID” countries that have had very few prior waves and, as a result, low infection-induced immunity. This category included countries in East Asia and the Pacific.
The researchers found that using booster vaccine doses can considerably contribute to mitigating the epidemic peaks in these countries, although it is possible that healthcare capacity may still be overwhelmed. The epidemic peaks of these countries will therefore be relatively higher than countries that have experienced previous pandemic waves.
Conclusions
The study findings demonstrate the significance of delivering booster vaccine doses as part of the public health response to the emergence of immune-escaping SARS-CoV-2 variants such as the Omicron variant in order to restore vaccine efficacy against these new viral strains. In scenarios where booster vaccine supply is limited, booster administration should be targeted at the high-risk groups rather than younger age groups to ensure that high-risk populations are offered maximum protection considering waning immunity.
In settings where health systems are still challenged, it might be necessary to maintain or reintroduce some NPIs to mitigate the adverse impacts caused by the Omicron variant.
With the Omicron variant rapidly replacing the Delta variant in many countries, emerging data on immunogenicity indicates a substantial reduction in NAT, while estimates of preliminary vaccine efficacy show a substantial decrease in protection from prior infection. Estimates from the present study demonstrate that this will potentially translate to notable reductions in efficacy against severe COVID-19 and related death.
Preliminary estimates of the severity of Omicron infection from South Africa, Canada, and the United Kingdom point to a considerable reduction compared to previous variants such as the Delta variant. However, this impact is likely dependent on the level of vaccination coverage, the population age distribution, and the extent of previous waves of infection.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
 Experimental two‑in‑one vaccine shows success in human LASSARAB trial
Experimental two‑in‑one vaccine shows success in human LASSARAB trial