Intrahepatic cholangiocarcinoma (iCCA), the second most common primary liver cancer after hepatocellular carcinoma, remains one of the most challenging malignancies to treat due to its highly concealed and heterogeneous nature. A collaborative team from BGI Genomics and Zhongshan Hospital of Fudan University has now charted the molecular “chaos” of iCCA, providing a navigational framework for more precise diagnosis and treatment. The research is published in Cell Reports Medicine.
A 1,341‑gene signature to cut sampling bias
A major barrier in iCCA treatment is its pronounced intratumoral heterogeneity. Cancer cells from different regions of the same tumor can exhibit markedly distinct molecular characteristics, meaning that a single biopsy often fails to capture the full biological landscape. The researchers found that current classification approaches misclassify more than one-quarter of tumors and up to two-thirds of immune profiles, depending on biopsy location.
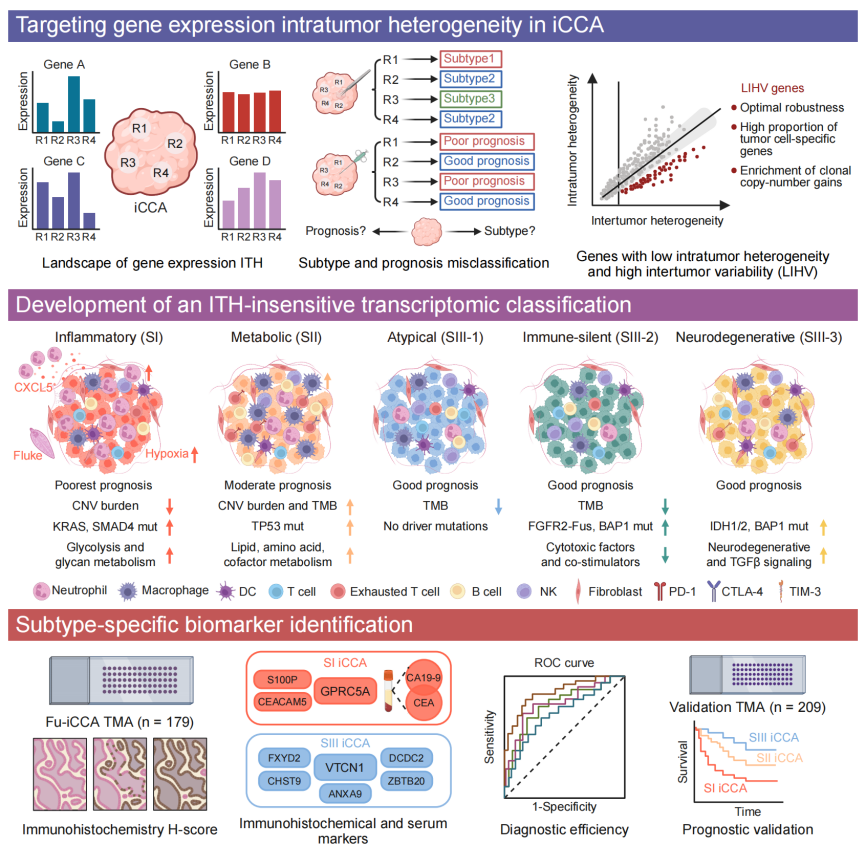
Figure 1. Molecular classification system of intrahepatic cholangiocarcinoma (iCCA). Image Credit: BGI Genomics
To address this challenge, the team identified a low-intratumor heterogeneity/high-intertumor variability (LIHV) gene set. This 1,341-gene signature focuses on markers that remain stable within an individual’s tumor but vary significantly between patients. By filtering out inconsistent "noise", the LIHV framework enables a more robust and reproducible classification of iCCA into five molecular subtypes, each associated with distinct therapeutic vulnerabilities:
Inflammatory subtype (SI): Associated with the poorest prognosis and enriched in large bile duct–type iCCA. These tumors frequently harbor KRAS and SMAD4 mutations and exhibit elevated serum CA19-9 and CEA levels. Their microenvironment is characterized by strong neutrophil infiltration, with chemokine CXCL5 playing a central role.
Metabolic subtype (SII): Displays the highest tumor mutation burden and elevated expression of multiple immune checkpoint molecules. Despite an immunosuppressive phenotype, this profile suggests potential sensitivity to immune checkpoint inhibitors and combination immunotherapies.
SIII group (SIII-1, SIII-2, SIII-3): Comprising atypical, immune-silent, and neurodegenerative subtypes, respectively, this group is primarily associated with small bile duct–type iCCA and generally shows better clinical outcomes. Distinct mutation patterns are observed, including enrichment of BAP1 mutations in SIII-2 and IDH1/2 mutations in SIII-3.
While previous studies have classified iCCA based on genetic alterations or tumor microenvironment features, this framework uniquely emphasizes genes that remain stable within tumors, thereby minimizing sampling bias and improving classification reliability.
Translating subtypes into therapeutic strategies
Beyond classification, the true clinical value of this framework lies in its ability to guide treatment decisions. For the inflammatory (SI) subtype, which is highly aggressive and often resistant to PD-1 blockade, the study demonstrates for the first time that HSP90 inhibitors can suppress tumor growth. Importantly, these agents appear to sensitize tumors to PD-1 therapy, suggesting a promising combination strategy for high-risk patients. In the neurodegenerative (SIII-3) subtype, tumors exhibit elevated expression of the immune checkpoint TIM-3. Experimental evidence indicates that dual blockade of PD-1 and TIM-3 is significantly more effective in controlling tumor progression than either therapy alone. The metabolic (SII) subtype presents a paradox: despite its immunosuppressive phenotype, it expresses high levels of multiple checkpoint molecules. This suggests that combination therapies targeting CTLA-4 and LAG3 may offer a viable strategy to overcome immune resistance. Although these findings are currently at the preclinical stage, they establish a structured foundation for future clinical trials tailored to subtype-specific molecular profiles.
Practical Biomarkers for Clinical Application
To facilitate clinical translation, the researchers identified accessible biomarkers that can serve as surrogate indicators for each subtype.
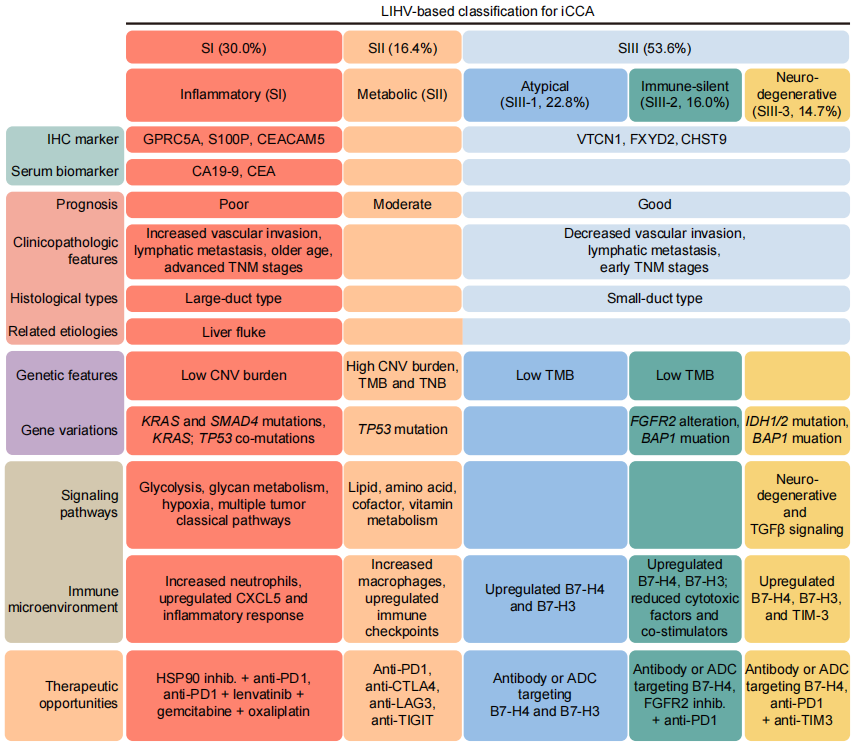
Figure 2. Summary diagram of iCCA molecular subtype characteristics and biomarkers. Image Credit: BGI Genomics
GPRC5A was identified as a specific marker for the inflammatory (SI) subtype, demonstrating a sensitivity of 71.4% and specificity of 88.9%. This marker may assist pathologists in identifying this aggressive subtype in routine histopathological evaluation.
VTCN1 (also known as B7-H4) was identified as a marker for the SIII group, with a sensitivity of 68.7% and specificity of 80.6%. Additionally, serum levels of CEA and CA19-9 may serve as non-invasive indicators of the inflammatory subtype, supporting integration of molecular classification into routine clinical workflows.
Toward Precision Oncology in iCCA
This study provides a comprehensive “roadmap” for navigating the biological complexity of iCCA by directly linking molecular subtypes to prognosis and targeted therapeutic strategies. The LIHV gene signature effectively overcomes the limitations imposed by tumor heterogeneity, enabling small biopsy samples to more accurately represent the entire tumor. Future work will focus on validating this framework across diverse patient populations and advancing subtype-guided therapies into clinical trials. By moving beyond one-size-fits-all approaches toward data-driven precision oncology, this roadmap holds promise for significantly improving survival outcomes and quality of life for patients with iCCA.
About BGI Genomics
BGI Genomics, headquartered in Shenzhen, China, is the world's leading integrated solutions provider of precision medicine. Our services cover more than 100 countries and regions, involving more than 2,300 medical institutions. In July 2017, as a subsidiary of BGI Group, BGI Genomics (300676.SZ) was officially listed on the Shenzhen Stock Exchange.
 Advancing Precision Medicine in Argentina, Brazil and Chile – BGI Update
Advancing Precision Medicine in Argentina, Brazil and Chile – BGI Update