As teplizumab opens the door to disease-modifying treatment, researchers say the next era of type 1 diabetes care may depend on protecting beta cells, calming autoimmune attack, and finding patients early enough to change the disease trajectory.
Review: New and emerging therapies in type 1 diabetes mellitus. Image Credit: rob9000 / Shutterstock
In a recent review published in The Journal of Clinical Investigation, researchers synthesized studies investigating emergent disease-modifying therapies for Type 1 diabetes mellitus (T1D) that aim to preserve endogenous beta-cell mass and actively promote or extend immunological tolerance, thereby providing a disease-modifying complement to conventional insulin replacement therapy for blood sugar control.
The review examines the clinical transition toward disease-modifying therapies, evaluating clinical trial data alongside novel beta-cell cytoprotective small molecules. Review findings highlight that blocking parallel inflammatory and cellular stress networks may offer a viable clinical pathway toward more durable metabolic benefit, potentially revolutionizing personalized treatment for future T1D patients.
Type 1 Diabetes Therapy Background
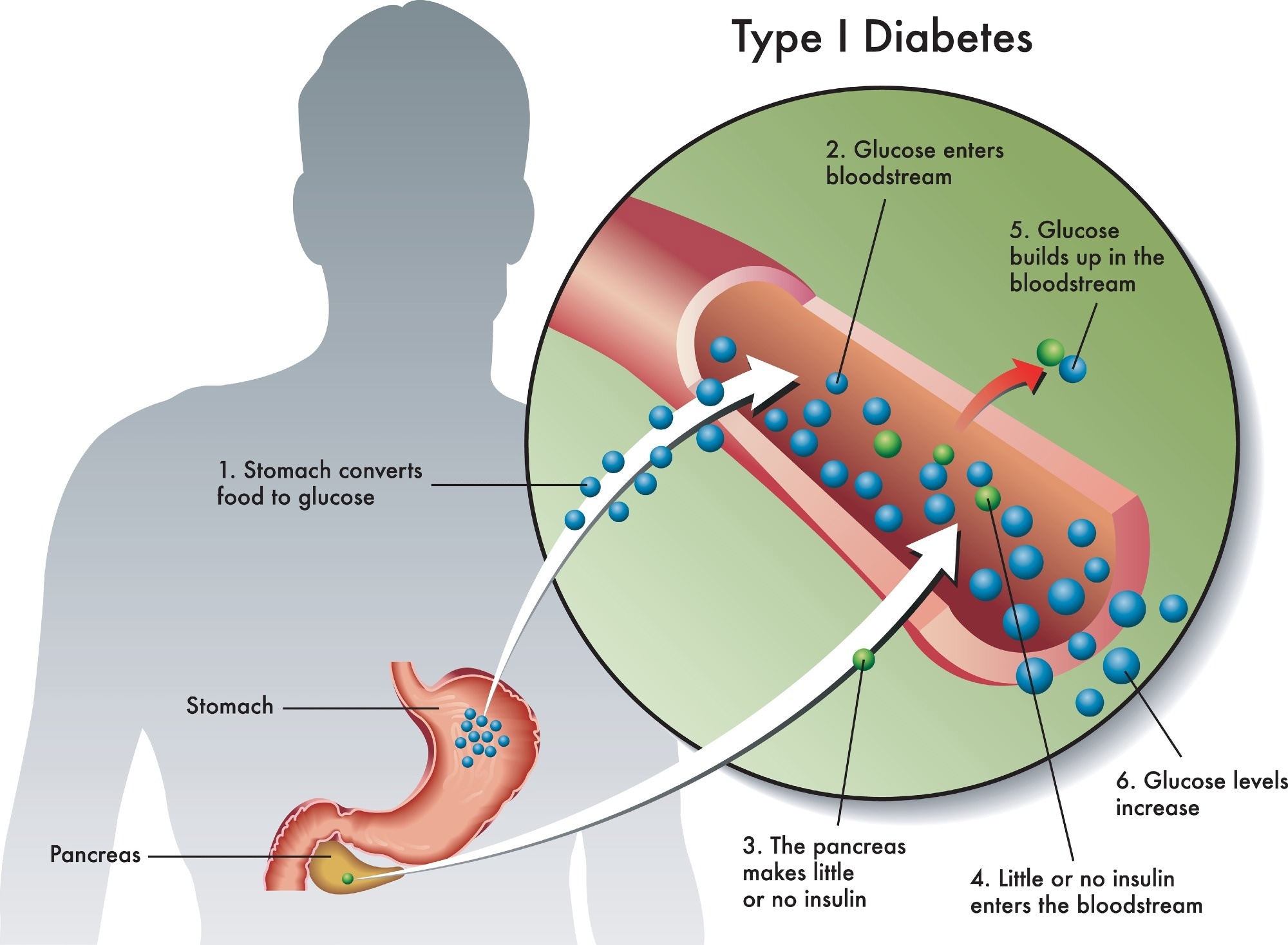
Since the discovery of insulin over a century ago, the management of type 1 diabetes (T1D) has predominantly relied on exogenous insulin injections to compensate for the patient’s loss of endogenous insulin-secreting beta cells.
However, long-term studies show that fewer than 25% of individuals with T1D consistently achieve recommended glycemic targets using standard methods such as continuous glucose monitoring and automated delivery algorithms. Most patients instead remain exposed to risks of severe hypoglycemia and multi-organ vascular complications.
These long-standing limitations underscore the need for therapeutic strategies that modify the underlying disease course rather than using insulin injections for symptomatic compensation.
Longitudinal natural history studies have defined T1D progression across a pre-symptomatic continuum divided into three metabolic stages. Stage 1 is marked by the presence of two or more islet autoantibodies with normal glucose tolerance; Stage 2 exhibits demonstrable glucose intolerance; and Stage 3 represents explicit metabolic decompensation meeting standard clinical diagnostic thresholds.
Notably, the median time to progression from Stage 2 to Stage 3 is roughly 2 years, with underlying beta-cell impairment consistently measurable at least 5 years prior to clinical diagnosis, highlighting a critical window that could be used to delay progression or alter the disease trajectory.
Disease-Modifying T1D Review Scope
The present review integrates data from preclinical animal models, human cellular lines, and multi-center clinical networks, focusing on emergent mechanisms that may delay or halt T1D progression.
The review’s methodology sought to contrast historical findings in non-obese diabetic (NOD) mice, characterized by robust, CD4+ T cell-dominated pancreatic inflammation, with direct analyses of human pancreatic tissues from organ donor programs.
Notably, human-derived data revealed a more modest insulitis dominated by CD8+ T cells, illustrating structural differences between rodents and humans and highlighting that historical evidence from NOD systems may not be directly translatable to human patients.
The review further evaluated the efficacy of various phase II and phase III clinical trials by focusing on core clinical endpoints, particularly the preservation of C-peptide, a validated biomarker of endogenous beta-cell function, alongside insulin requirements and glycated hemoglobin (HbA1c) levels. This framework enabled the review to elucidate how specific therapeutic agents are designed to disrupt the destructive cycle between the endocrine and immune systems.
Teplizumab and Beta-Cell Protection Findings
The review highlights the regulatory approval of teplizumab, an anti-CD3 monoclonal antibody that delivers a partial agonist signal to T cells, as a major milestone in the treatment of T1D.
In a clinical trial of high-risk Stage 2 patients, a single 14-day course of teplizumab was found to delay clinical Stage 3 diagnosis by a median of 24 to 48 months, with a maximum of 60 months in follow-up analyses. These benefits were attributed to teplizumab triggering a “partial exhaustion” phenotype in destructive CD8+ T cells.
Additionally, therapies targeting beta-cell-intrinsic stress pathways showed promise. A 26-week regimen of imatinib, an Abelson murine leukemia viral oncogene homolog (Abl) kinase inhibitor, was shown to improve C-peptide during treatment, although the effect was not sustained to 24 months.
However, safety evaluations revealed that 71% of treated participants experienced grade-2 or worse adverse events, compared with 59% on placebo, indicating the need for further safety-focused development before these benefits can be more broadly translated.
The calcium channel blocker verapamil also showed modest C-peptide preservation in pediatric trials involving children and adolescents aged 8 to 17 years by inhibiting thioredoxin-interacting protein (TXNIP) expression. However, the drug failed to show significant clinical benefit in an adult cohort, and the absence of a circulating TXNIP pharmacodynamic signal complicates mechanistic interpretation.
Furthermore, therapies targeting inflammatory cytokines and cytokine signaling have also yielded notable data: a Phase II trial of golimumab, an anti-tumor necrosis factor-alpha (anti-TNF-α) monoclonal antibody (n = 84), and a trial evaluating baricitinib, a Janus kinase (JAK) 1 and 2 inhibitor (n = 91), both of which documented preserved C-peptide responses and reduced exogenous insulin requirements.
T1D Combination Therapy Implications
The present review reveals that while monotherapies provide temporary delays in metabolic decline, they have not yet demonstrated a permanent reversal of autoimmune pathology.
The data strongly imply that establishing long-term metabolic remission will necessitate sequential or combination regimens. An immediate example is the ongoing TrialNet study pairing the anti-CD20 B-cell depleting antibody rituximab with the costimulatory blocker abatacept to systematically disrupt adaptive T-cell reactivation.
Consequently, the authors recommend that future screening frameworks be adopted by widespread primary care practices. Proactively identifying individuals during Stages 1 and 2 enables therapeutic deployment before substantial beta-cell decline, thereby potentially reshaping the disease trajectory.
Download your PDF copy by clicking here.
Journal reference:
- Herold, K. C., & Evans-Molina, C. (2026). New and emerging therapies in type 1 diabetes mellitus. The Journal of Clinical Investigation, 136(10), Article e205520. DOI: 10.1172/JCI205520. https://www.jci.org/articles/view/205520
 Scientists uncover protein-folding mechanism linked to diabetes progression
Scientists uncover protein-folding mechanism linked to diabetes progression